

Midwife-Led Versus Obstetrician-Led Perinatal Care for Low-Risk Pregnancy: A Systematic Review and Meta-Analysis of 1.4 Million Pregnancies
- PMID: 39597773
- PMCID: PMC11594941
- DOI: 10.3390/jcm13226629
Midwife-Led Versus Obstetrician-Led Perinatal Care for Low-Risk Pregnancy: A Systematic Review and Meta-Analysis of 1.4 Million Pregnancies
Abstract
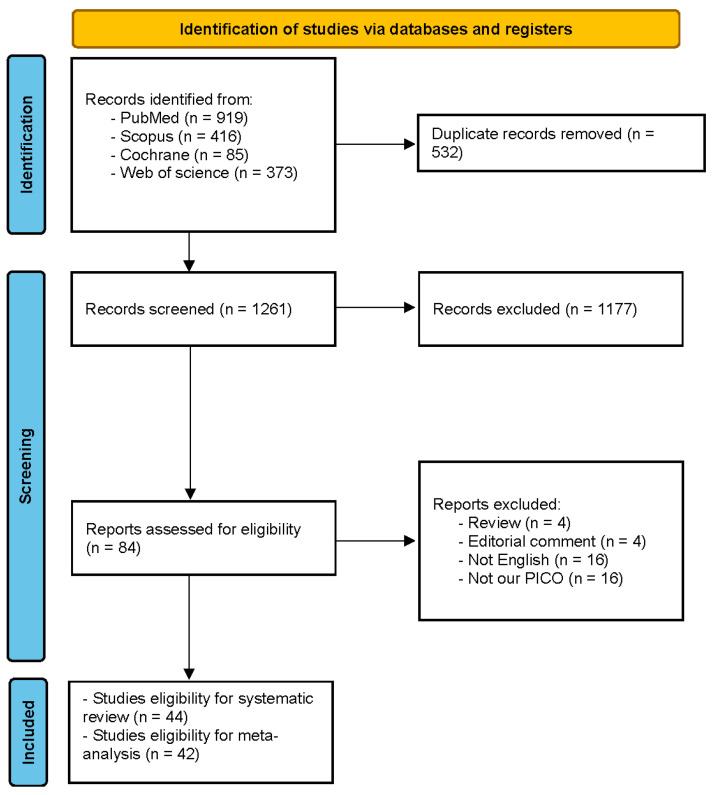
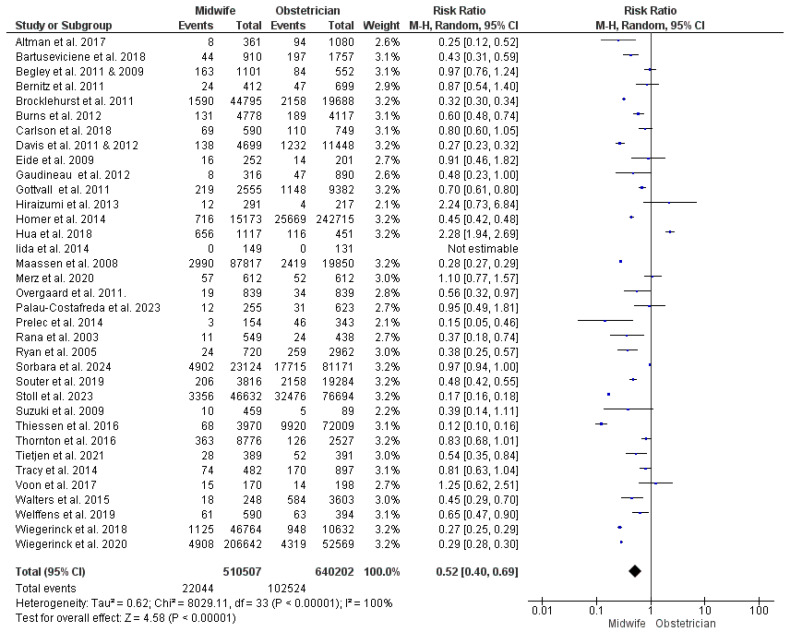
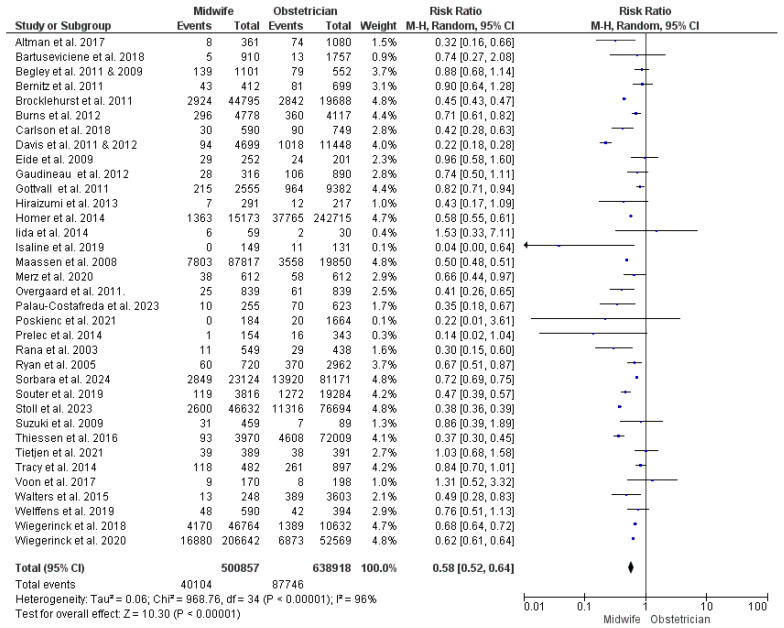
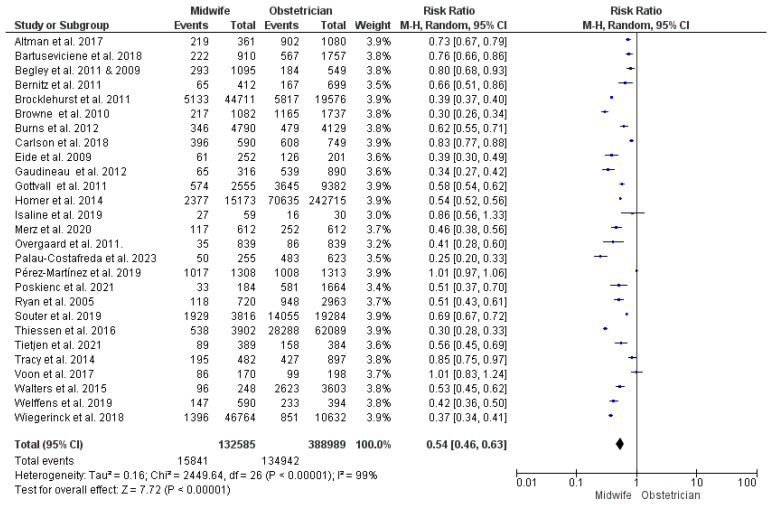
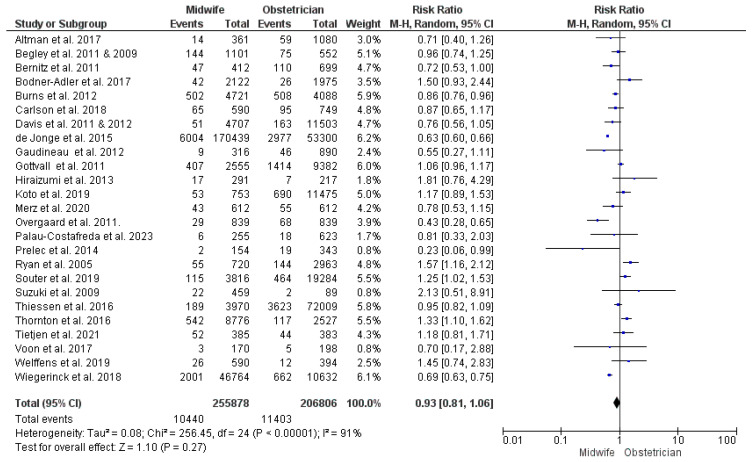
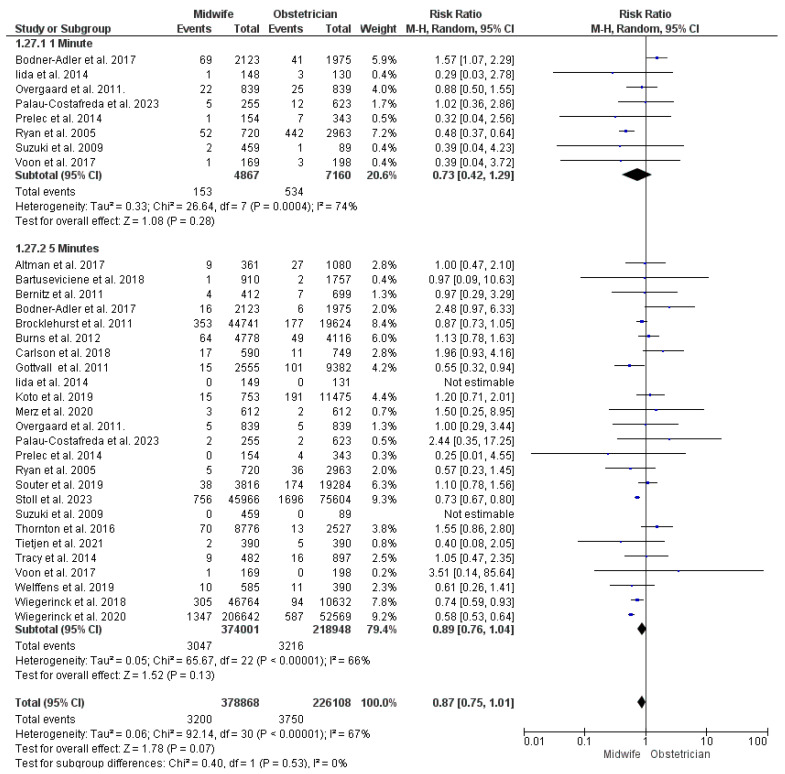
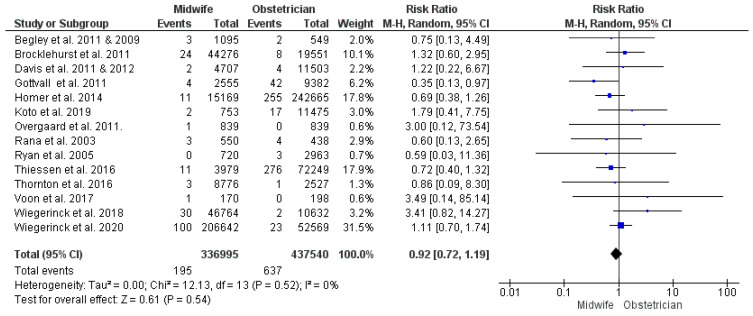
Background: The optimum model of perinatal care for low-risk pregnancies has been a topic of debate. Obstetrician-led care tends to perform unnecessary interventions, whereas the quality of midwife-led care has been subject to debate. This review aimed to assess whether midwife-led care reduces childbirth intervention and whether this comes at the expense of maternal and neonatal wellbeing. Methods: PubMed, Scopus, Cochrane Library, and Web of Science were systematically searched for relevant studies. Studies were checked for eligibility by screening the titles, abstracts, and full texts. We performed meta-analyses using the inverse variance method using RevMan software version 5.3. We pooled data using the risk ratio and mean difference with the 95% confidence interval. Results: This review included 44 studies with 1,397,320 women enrolled. Midwife-led care carried a lower risk of unplanned cesarean and instrumental vaginal deliveries, augmentation of labor, epidural/spinal analgesia, episiotomy, and active management of labor third stage. Women who received midwife-led care had shorter hospital stays and lower risks of infection, manual removal of the placenta, blood transfusion, and intensive care unit (ICU) admission. Furthermore, neonates delivered under midwife-led care had lower risks of acidosis, asphyxia, transfer to specialist care, and ICU admission. Postpartum hemorrhage, perineal tears, APGAR score < 7, and other outcomes were comparable between the two models of management. Conclusions: Midwife-led care reduced childbirth interventions with favorable maternal and neonatal outcomes in most cases. We recommend assigning low-risk pregnancies to midwife-led perinatal care in health systems with infrastructure allowing for smooth transfer when complications arise. Further research is needed to reflect the situation in low-resource countries.
Keywords: childbirth; low-risk; meta-analysis; midwife; obstetrician.
Conflict of interest statement
Author Fahad M. Almutairi was employed by Health Holding Company, Ministry of Health, Jeddah, Saudi Arabia. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
