

Automatic Image Registration Provides Superior Accuracy Compared with Surface Matching in Cranial Navigation
- PMID: 39599122
- PMCID: PMC11597983
- DOI: 10.3390/s24227341
Automatic Image Registration Provides Superior Accuracy Compared with Surface Matching in Cranial Navigation
Abstract
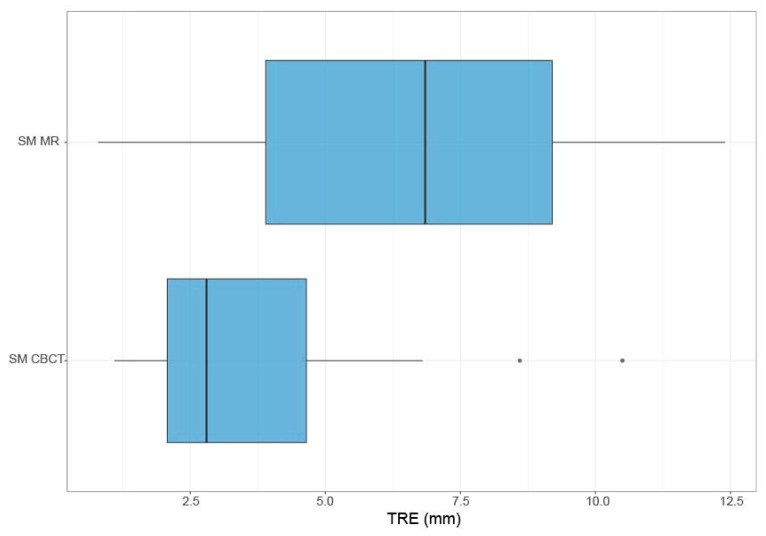
Objective: The precision of neuronavigation systems relies on the correct registration of the patient's position in space and aligning it with radiological 3D imaging data. Registration is usually performed by the acquisition of anatomical landmarks or surface matching based on facial features. Another possibility is automatic image registration using intraoperative imaging. This could provide better accuracy, especially in rotated or prone positions where the other methods may be difficult to perform. The aim of this study was to validate automatic image registration (AIR) using intraoperative cone-beam computed tomography (CBCT) for cranial neurosurgical procedures and compare the registration accuracy to the traditional surface matching (SM) registration method based on preoperative MRI. The preservation of navigation accuracy throughout the surgery was also investigated.
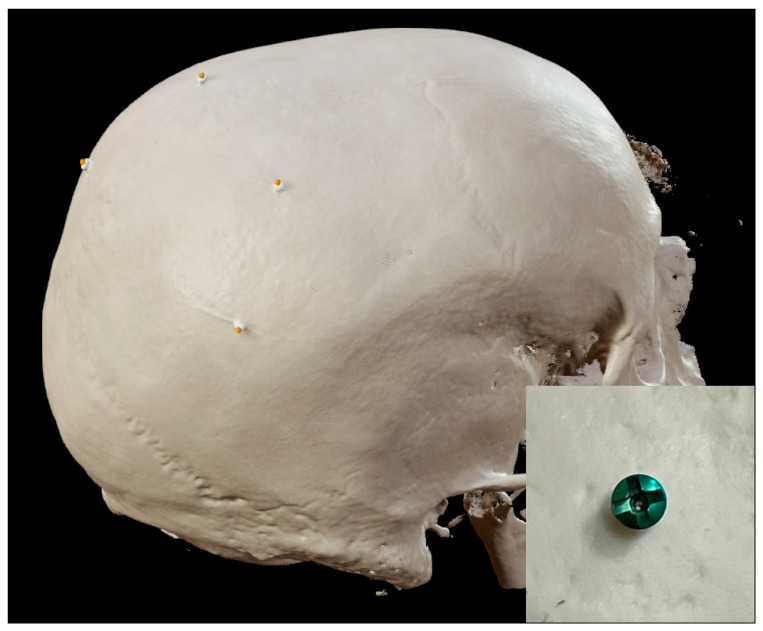
Methods: Adult patients undergoing intracranial tumor surgery were enrolled after consent. A standard SM registration was performed, and reference points were acquired. An AIR was then performed, and the same reference points were acquired again. Accuracy was calculated based on the referenced and acquired coordinates of the points for each registration method. The reference points were acquired before and after draping and at the end of the procedure to assess the persistency of accuracy.
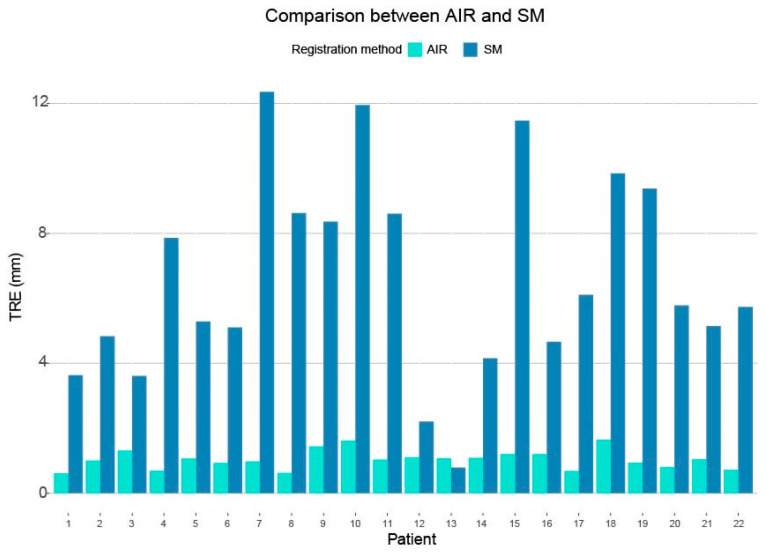
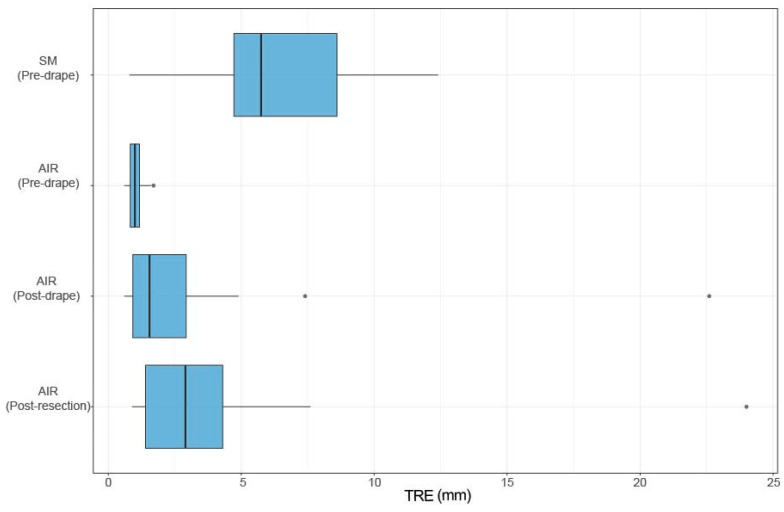
Results: In total, 22 patients were included. The mean accuracy was 6.6 ± 3.1 mm for SM registration and 1.0 ± 0.3 mm for AIR. The AIR was superior to the SM registration (p < 0.0001), with a mean improvement in accuracy of 5.58 mm (3.71-7.44 mm 99% CI). The mean accuracy for the AIR registration pre-drape was 1.0 ± 0.3 mm. The corresponding accuracies post-drape and post-resection were 2.9 ± 4.6 mm and 4.1 ± 4.9 mm, respectively. Although a loss of accuracy was identified between the preoperative and end-of-procedure measurements, there was no statistically significant decline during surgery.
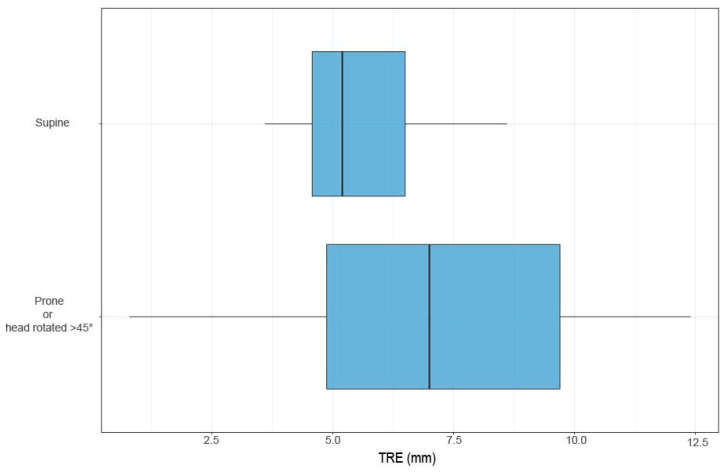
Conclusions: AIR for cranial neuronavigation consistently delivered greater accuracy than SM and should be considered the new gold standard for patient registration in cranial neuronavigation. If intraoperative imaging is a limited resource, AIR should be prioritized in rotated or prone position procedures, where the benefits are the greatest.
Keywords: CBCT; accuracy; automatic image registration; neurosurgery; patient tracking; reference frame; surface matching; surgical navigation.
Conflict of interest statement
None of the authors who are affiliated with clinical institutions (H.F., M.J., L.A., J.B.J., G.B., V.G.E.-H., E.E., A.E.-T. and O.P.) have financial interests in the subject matter, materials, or equipment or with any competing materials and did not receive any payments from Brainlab. A.E.-T. was a consultant for Brainlab during the data collection and until September 2022, when the consultancy was terminated. The other authors affiliated with Brainlab (L.C., M.C. and S.H.) have financial interests in the subject matter, materials, and equipment in the sense that they are employees of Brainlab. The extent of influence on the data, manuscript structure, and manuscript conclusions by these authors and/or Brainlab was limited to technical knowledge and support for the experiments as well as performing technical analysis of image data. Authors without conflicts of interest had full control of all data labeling, data analysis, information submitted for publication, and the overall conclusions drawn in the manuscript.
Figures



Similar articles
-
Automatic image registration on intraoperative CBCT compared to Surface Matching registration on preoperative CT for spinal navigation: accuracy and workflow.Int J Comput Assist Radiol Surg. 2024 Apr;19(4):665-675. doi: 10.1007/s11548-024-03076-4. Epub 2024 Feb 20. Int J Comput Assist Radiol Surg. 2024. PMID: 38378987 Free PMC article.
-
Automatic image-to-world registration based on x-ray projections in cone-beam CT-guided interventions.Med Phys. 2009 May;36(5):1800-12. doi: 10.1118/1.3117609. Med Phys. 2009. PMID: 19544799 Free PMC article.
-
Reliable navigation registration in cranial and spine surgery based on intraoperative computed tomography.Neurosurg Focus. 2019 Dec 1;47(6):E11. doi: 10.3171/2019.8.FOCUS19621. Neurosurg Focus. 2019. PMID: 31786552
-
Multimodal image registration for preoperative planning and image-guided neurosurgical procedures.Neurosurg Clin N Am. 2011 Apr;22(2):197-206, viii. doi: 10.1016/j.nec.2010.12.001. Neurosurg Clin N Am. 2011. PMID: 21435571 Free PMC article. Review.
-
IBIS: an OR ready open-source platform for image-guided neurosurgery.Int J Comput Assist Radiol Surg. 2017 Mar;12(3):363-378. doi: 10.1007/s11548-016-1478-0. Epub 2016 Aug 31. Int J Comput Assist Radiol Surg. 2017. PMID: 27581336 Review.
References
-
- Burström G., Nachabe R., Homan R., Hoppenbrouwers J., Holthuizen R., Persson O., Edström E., Elmi-Terander A. Frameless Patient Tracking with Adhesive Optical Skin Markers for Augmented Reality Surgical Navigation in Spine Surgery. Spine (Phila Pa 1976) 2020;45:1598–1604. doi: 10.1097/BRS.0000000000003628. - DOI - PubMed
-
- Frisk H., Burström G., Persson O., El-Hajj V.G., Coronado L., Hager S., Edström E., Elmi-Terander A. Automatic image registration on intraoperative CBCT compared to Surface Matching registration on preoperative CT for spinal navigation: Accuracy and workflow. Int. J. Comput. Assist. Radiol. Surg. 2024;19:665–675. doi: 10.1007/s11548-024-03076-4. - DOI - PMC - PubMed
-
- Mascott C.R., Sol J.C., Bousquet P., Lagarrigue J., Lazorthes Y., Lauwers-Cances V. Quantification of true in vivo (application) accuracy in cranial image-guided surgery: Influence of mode of patient registration. Neurosurgery. 2006;59:ONS146–ONS156. doi: 10.1227/01.NEU.0000220089.39533.4E. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
