

Prevalence Rates of Abdominal Obesity, High Waist-to-Height Ratio and Excess Adiposity, and Their Associated Cardio-Kidney-Metabolic Factors: SIMETAP-AO Study
- PMID: 39599733
- PMCID: PMC11597375
- DOI: 10.3390/nu16223948
Prevalence Rates of Abdominal Obesity, High Waist-to-Height Ratio and Excess Adiposity, and Their Associated Cardio-Kidney-Metabolic Factors: SIMETAP-AO Study
Abstract
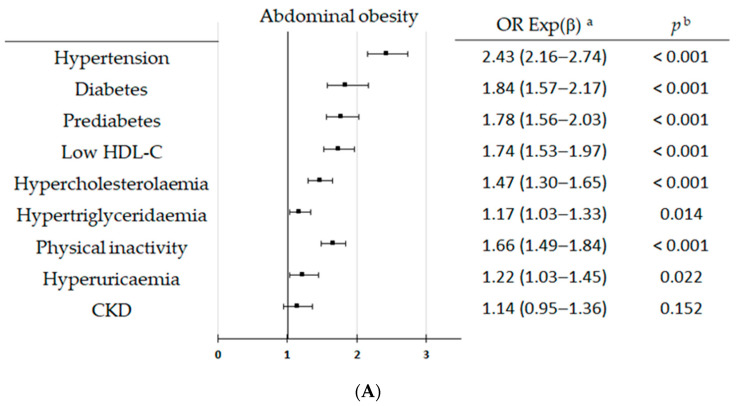
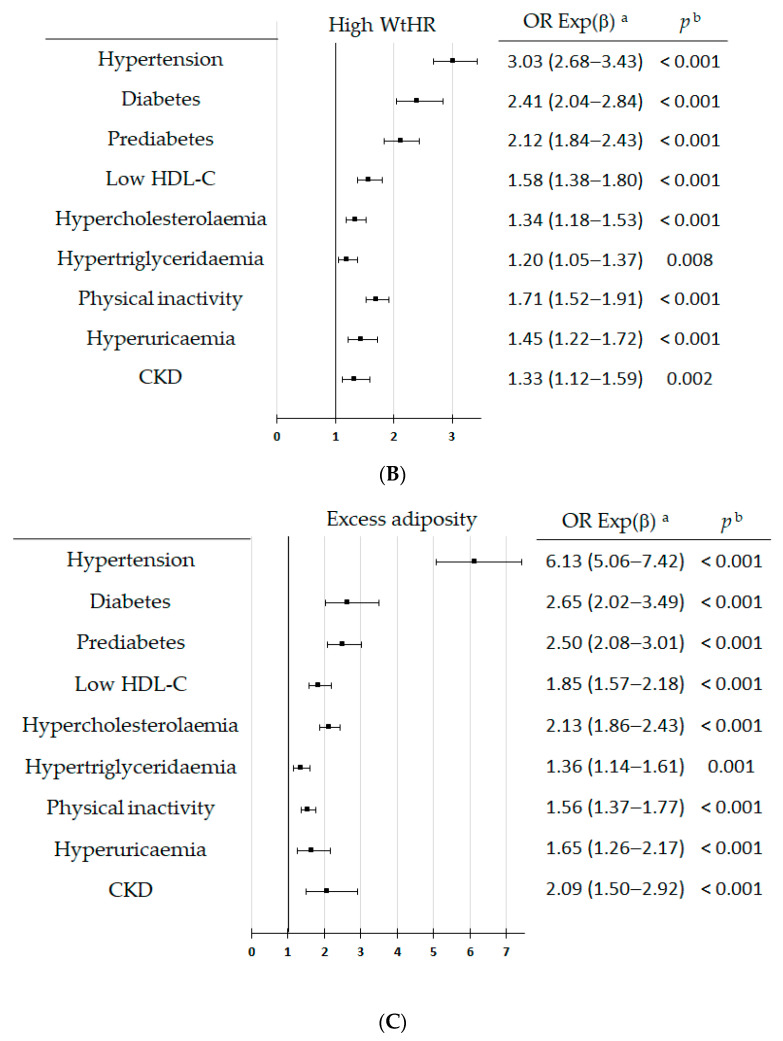
Background/objective: In addition to obesity, adiposity and abdominal obesity (AO) are parameters included in the cardiovascular-kidney-metabolic (CKM) syndrome. However, their prevalence and association with the other CKM factors have been less studied. Our study aimed to determine the prevalence rates of AO, high waist-to-height ratio (WtHR), and excess adiposity (EA), and to compare their associations with CKM factors.
Methods: A cross-sectional observational study was conducted with a random population-based sample of 6,588 study subjects between 18 and 102 years of age. Crude and sex- and age-adjusted prevalence rates of AO, high-WtHR, and EA were calculated, and their associations with CKM variables were assessed by bivariate and multivariate analyses.
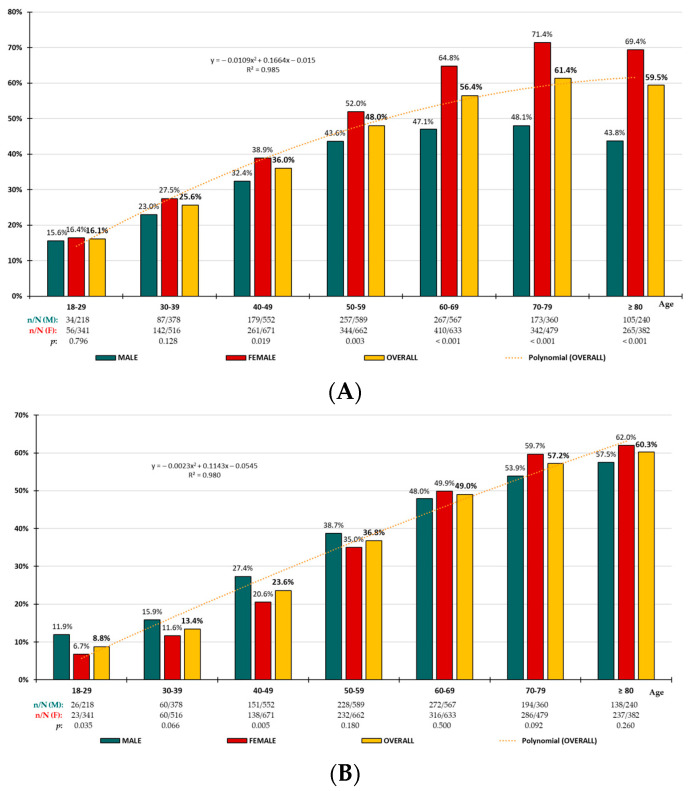
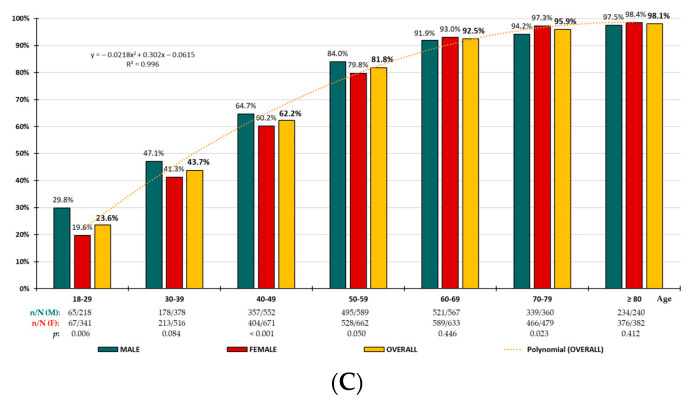
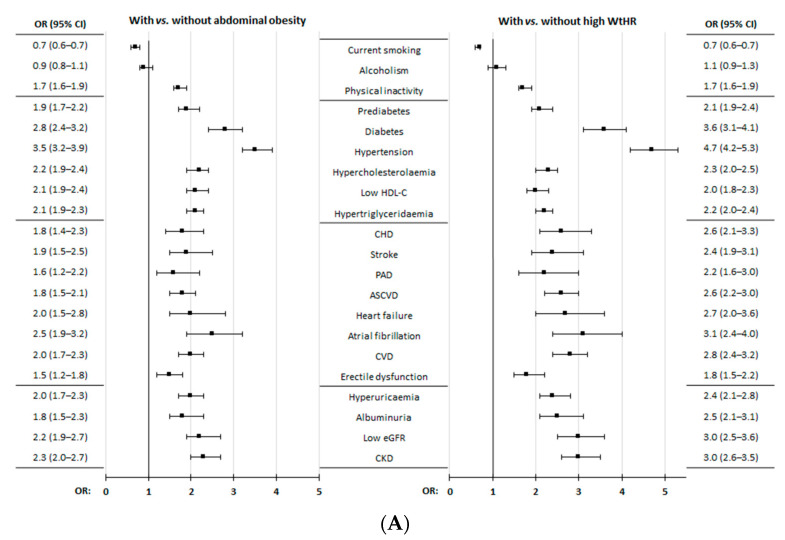
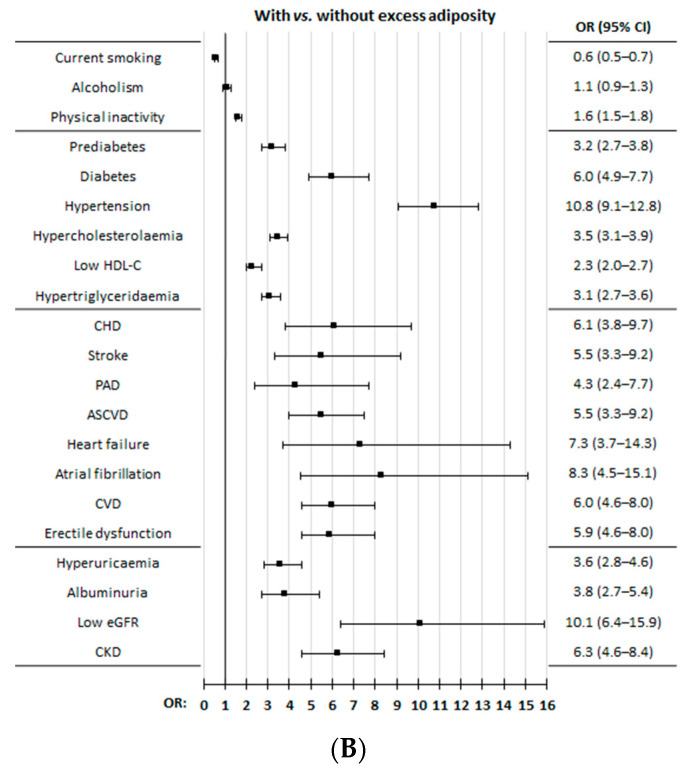
Results: The adjusted prevalence rates for AO, high-WtHR, and EA were 39.6% (33.6% in men; 44.9% in women), 30.6% (31.1% in men; 30.6% in women), and 65.6% (65.6% in men; 65.3% in women), respectively, and they increased with age. The main independent factors associated with AO, high-WtHR, and EA were hypertension, diabetes, prediabetes, low HDL-C, hypercholesterolaemia, hypertriglyceridemia, physical inactivity, hyperuricemia, and chronic kidney disease.
Conclusions: Two-thirds of the adult population have EA, one-third have AO, and one-third have high-WtHR. These findings support that the other factors of CKM syndrome, in addition to hyperuricemia and physical inactivity, show an independent association with these adiposity-related variables.
Keywords: abdominal obesity; adiposity; adults; cardiovascular risk factors; prevalence; waist-to-height ratio.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
From Metabolic Syndrome to Cardio-Kidney-Metabolic Syndrome in the SIMETAP Study: Prevalence Rates of Metabolic Syndrome and Its Independent Associations with Cardio-Renal-Metabolic Disorders Other than Its Defining Criteria.Biomedicines. 2025 Feb 28;13(3):590. doi: 10.3390/biomedicines13030590. Biomedicines. 2025. PMID: 40149567 Free PMC article.
-
Waist-to-height ratio is a useful indicator of cardio-metabolic risk in South Africa.Fam Pract. 2020 Feb 19;37(1):36-42. doi: 10.1093/fampra/cmz044. Fam Pract. 2020. PMID: 31504474
-
Association Between Pediatric Psoriasis and Waist-to-Height Ratio in the Absence of Obesity: A Multicenter Australian Study.JAMA Dermatol. 2016 Dec 1;152(12):1314-1319. doi: 10.1001/jamadermatol.2016.3432. JAMA Dermatol. 2016. PMID: 27681388
-
Obesity, central adiposity and cardiometabolic risk factors in children and adolescents: a family-based study.Pediatr Obes. 2014 Jun;9(3):e58-e62. doi: 10.1111/j.2047-6310.2014.218.x. Epub 2014 Mar 27. Pediatr Obes. 2014. PMID: 24677702 Free PMC article. Review.
-
An overview of cardiovascular-kidney-metabolic syndrome.Am J Manag Care. 2024 Dec;30(10 Suppl):S181-S188. doi: 10.37765/ajmc.2024.89670. Am J Manag Care. 2024. PMID: 39705194 Review.
Cited by
-
Association between body roundness index and advanced cardiovascular-kidney-metabolic syndrome.Front Nutr. 2025 Jul 30;12:1623766. doi: 10.3389/fnut.2025.1623766. eCollection 2025. Front Nutr. 2025. PMID: 40808842 Free PMC article.
References
-
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in underweight and obesity from 1990 to 2022: A pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. Lancet. 2024;403:1027–1050. doi: 10.1016/S0140-6736(23)02750-2. - DOI - PMC - PubMed
-
- Ministerio de Sanidad Porcentaje de Personas con Obesidad, Por Sexo Según Comunidad Autónoma. [(accessed on 22 September 2024)]; Available online: https://www.sanidad.gob.es/estadEstudios/sanidadDatos/tablas/tabla10.htm.
-
- Gutiérrez-González E., García-Solano M., Pastor-Barriuso R., Fernández de Larrea-Baz N., Rollán-Gordo A., Peñalver-Argüeso B., Peña-Rey I., Pollán M., Pérez-Gómez B., ENE-COVID Study Group A nation-wide analysis of socioeconomic and geographical disparities in the prevalence of obesity and excess weight in children and adolescents in Spain: Results from the ENE-COVID study. Pediatr. Obes. 2024;19:e13085. doi: 10.1111/ijpo.13085. - DOI - PubMed
-
- WHO Consultation on Obesity . Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation. Volume 894. World Health Organization; Geneva, Switzerland: 2000. [(accessed on 22 September 2024)]. (WHO technical report series). Available online: https://apps.who.int/iris/handle/10665/42330. - PubMed
-
- Koskinas K.C., Van Craenenbroeck E.M., Antoniades C., Blüher M., Gorter T.M., Hanssen H., Marx N., A McDonagh T., Mingrone G., Rosengren A., et al. ESC Scientific Document Group. Obesity and cardiovascular disease: An ESC clinical consensus statement. Eur. Heart J. 2024;45:4063–4098. doi: 10.1093/eurheartj/ehae508. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
