

New cardiovascular biomarkers in patients with advanced cancer - A prospective study comparing MR-proADM, MR-proANP, copeptin, high-sensitivity troponin T and NT-proBNP
- PMID: 39600145
- PMCID: PMC12260322
- DOI: 10.1002/ejhf.3497
New cardiovascular biomarkers in patients with advanced cancer - A prospective study comparing MR-proADM, MR-proANP, copeptin, high-sensitivity troponin T and NT-proBNP
Abstract
Aims: Traditional cardiovascular (CV) biomarkers (high-sensitivity troponinT [hsTnT] and N-terminal pro-B-type natriuretic peptide [NT-proBNP]) are important to monitor cancer patients' cardiac function and to assess prognosis. Newer CV biomarkers (mid-regional pro-adrenomedullin [MR-proADM], C-terminal pro-arginine vasopressin [copeptin], and mid-regional pro-atrial natriuretic peptide [MR-proANP]) might outperform traditional biomarkers.
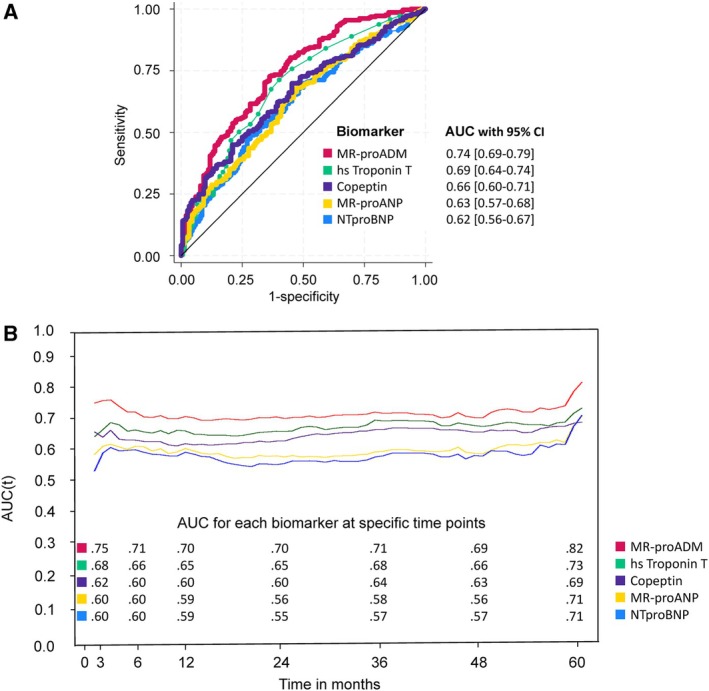
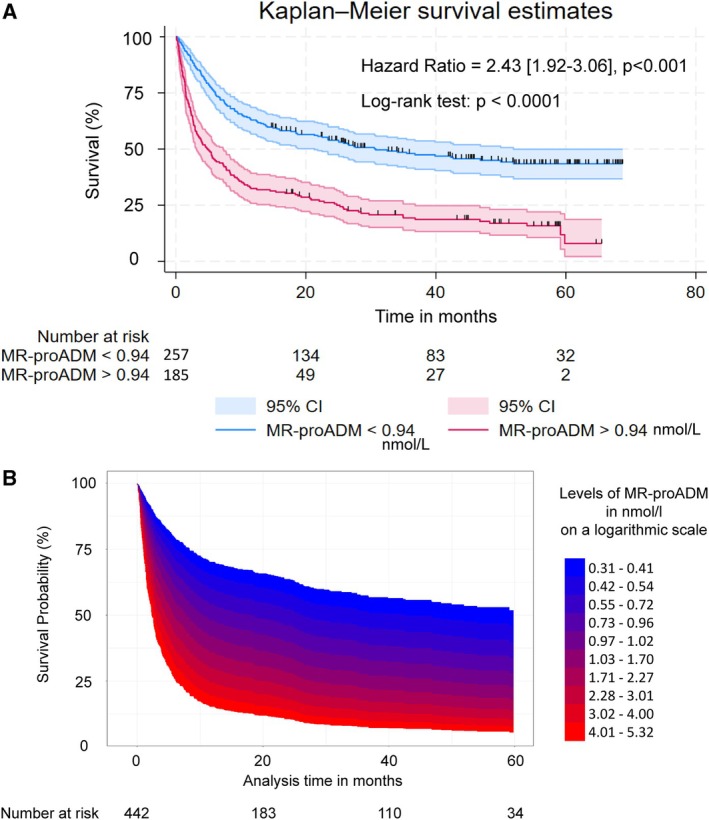
Methods and results: Overall, 442 hospitalized cancer patients without significant CV disease or current infection were enrolled (61 ± 15 years, 52% male, advanced cancer stage: 85%) and concentrations of CV biomarkers were analysed. Differences in echocardiographic, clinical, laboratory parameters were assessed. Patients were followed for up to 69 months for all-cause mortality. In univariable analyses, MR-proADM, hsTnT, copeptin, MR-proANP, and NT-proBNP predicted all-cause mortality. In multivariable analyses (adjusted for sex, age, Eastern Cooperative Oncology Group performance status, estimated glomerular filtration rate [eGFR], C-reactive protein, anti-cancer therapy, reason for hospitalization, cancer stage and type), only MR-proADM remained an independent predictor of mortality (MR-proADM per 1 ln: hazard ratio [HR] 2.27, 95% confidence interval [CI] 1.47-3.50], p < 0.001). MR-proADM had the highest area under the curve (AUC) using receiver operating characteristic analysis (AUC [95% CI] 0.74 [0.69-0.79]; hsTnT: AUC 0.69; copeptin: AUC 0.66; MR-proANP: AUC 0.63; NT-proBNP: AUC 0.62). Optimal cut-point for mortality prediction with MR-proADM was 0.94 nmol/L (HR 2.43 [95% CI 1.92-3.06], p < 0.001). Patients with MR-proADM >0.94 nmol/L were older, more often had cancer stage IV, showed reduced performance status, eGFR, haemoglobin, diastolic left ventricular function, and elevated systolic pulmonary artery pressure.
Conclusion: MR-proADM is an independent predictor of mortality in advanced stage, hospitalized cancer patients without significant CV disease or current infection. The optimal MR-proADM cut-point for mortality prediction was 0.94 nmol/L with hazards for mortality being approximately 2.5 times higher. There was a continuous increase in mortality risk with stepwise increase of MR-proADM concentrations. Elevated concentrations of MR-proADM were also associated with reduced performance status and mildly reduced left ventricular diastolic function as well as higher age and more often cancer stage IV.
Keywords: Cardiovascular biomarkers; Cardio‐oncology; Diastolic dysfunction; MR‐proADM; Mortality.
© 2024 The Author(s). European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures
Similar articles
-
Cardiovascular biomarkers in patients with cancer and their association with all-cause mortality.Heart. 2015 Dec;101(23):1874-80. doi: 10.1136/heartjnl-2015-307848. Epub 2015 Sep 28. Heart. 2015. PMID: 26416836
-
Mid-regional pro-atrial natriuretic peptide and pro-adrenomedullin testing for the diagnostic and prognostic evaluation of patients with acute dyspnoea.Eur Heart J. 2012 Sep;33(17):2197-205. doi: 10.1093/eurheartj/ehs136. Epub 2012 May 29. Eur Heart J. 2012. PMID: 22645194 Free PMC article.
-
Association of High-Sensitivity Troponin T and I Blood Concentrations With All-Cause Mortality and Cardiovascular Outcome in Stable Patients-Results From the INTERCATH Cohort.J Am Heart Assoc. 2022 Sep 6;11(17):e024516. doi: 10.1161/JAHA.121.024516. Epub 2022 Jul 19. J Am Heart Assoc. 2022. PMID: 35862141 Free PMC article.
-
Prognostic value of mid-regional pro-adrenomedullin (MR-proADM) in patients with community-acquired pneumonia: a systematic review and meta-analysis.BMC Infect Dis. 2016 May 26;16:232. doi: 10.1186/s12879-016-1566-3. BMC Infect Dis. 2016. PMID: 27230573 Free PMC article.
-
Diagnostic Accuracy of Natriuretic Peptides for Heart Failure in Patients with Pleural Effusion: A Systematic Review and Updated Meta-Analysis.PLoS One. 2015 Aug 5;10(8):e0134376. doi: 10.1371/journal.pone.0134376. eCollection 2015. PLoS One. 2015. PMID: 26244664 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
