

Social Vulnerability, Intervention Utilization, and Outcomes in US Adults Hospitalized With Influenza
- PMID: 39602116
- PMCID: PMC11702903
- DOI: 10.1001/jamanetworkopen.2024.48003
Social Vulnerability, Intervention Utilization, and Outcomes in US Adults Hospitalized With Influenza
Abstract
Importance: Seasonal influenza is associated with substantial disease burden. The relationship between census tract-based social vulnerability and clinical outcomes among patients with influenza remains unknown.
Objective: To characterize associations between social vulnerability and outcomes among patients hospitalized with influenza and to evaluate seasonal influenza vaccine and influenza antiviral utilization patterns across levels of social vulnerability.
Design, setting, and participants: This retrospective repeated cross-sectional study was conducted among adults with laboratory-confirmed influenza-associated hospitalizations from the 2014 to 2015 through the 2018 to 2019 influenza seasons. Data were from a population-based surveillance network of counties within 13 states. Data analysis was conducted in December 2023.
Exposure: Census tract-based social vulnerability.
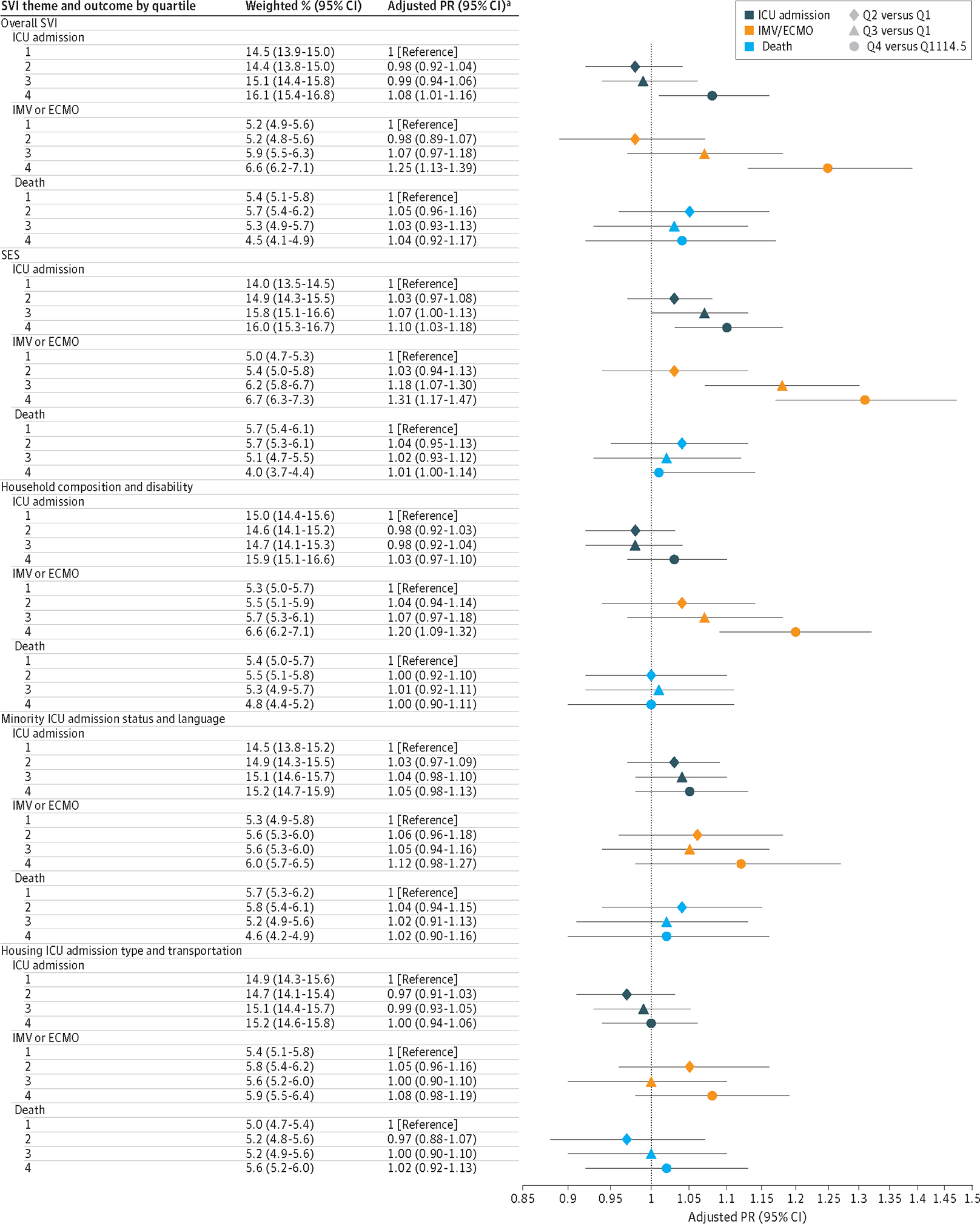
Main outcomes and measures: Associations between census tract-based social vulnerability and influenza outcomes (intensive care unit admission, invasive mechanical ventilation and/or extracorporeal membrane oxygenation support, and 30-day mortality) were estimated using modified Poisson regression as adjusted prevalence ratios. Seasonal influenza vaccine and influenza antiviral utilization were also characterized across levels of social vulnerability.
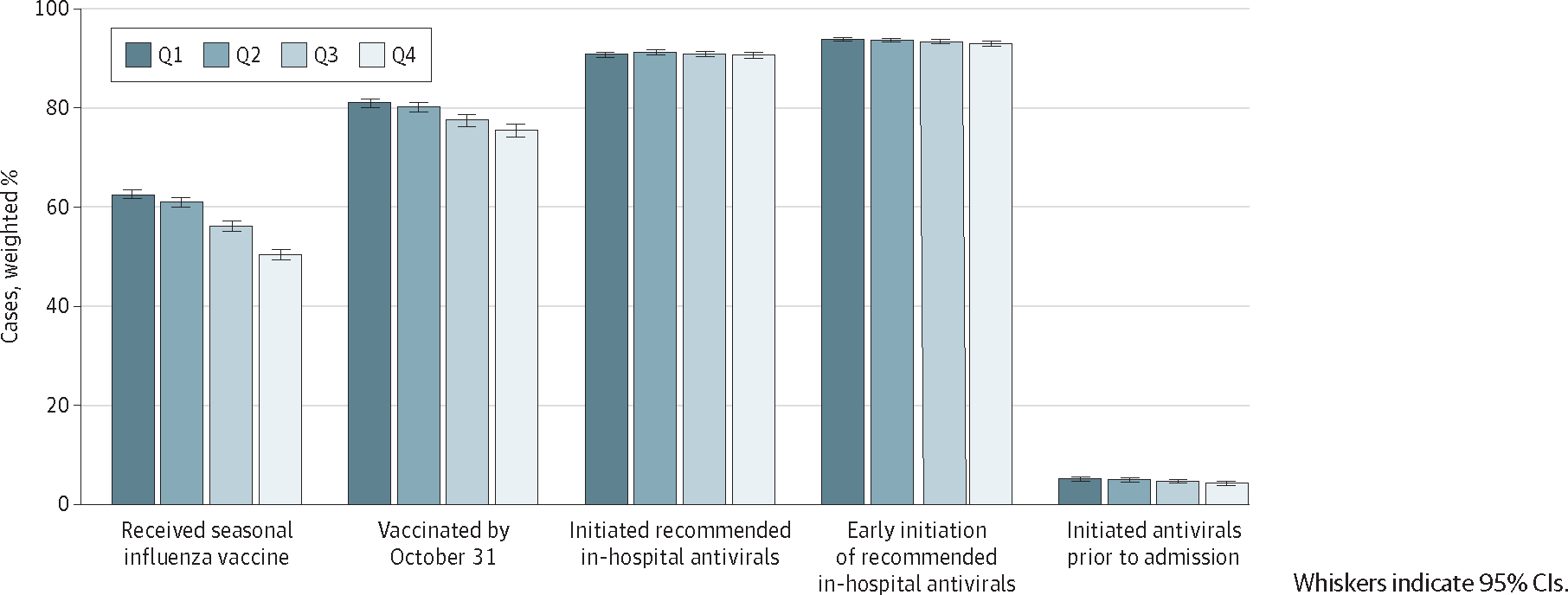
Results: Among 57 964 sampled cases, the median (IQR) age was 71 (58-82) years; 55.5% (95% CI, 51.5%-56.0%) were female; 5.2% (5.0%-5.4%) were Asian or Pacific Islander, 18.3% (95% CI, 18.0%-18.6%) were Black or African American, and 64.6% (95% CI, 64.2%-65.0%) were White; and 6.6% (95% CI, 6.4%-68%) were Hispanic or Latino and 74.7% (95% CI, 74.3%-75.0%) were non-Hispanic or Latino. High social vulnerability was associated with higher prevalence of invasive mechanical ventilation and/or extracorporeal membrane oxygenation support (931 of 13 563 unweighted cases; adjusted prevalence ratio [aPR], 1.25 [95% CI, 1.13-1.39]), primarily due to socioeconomic status (790 of 11 255; aPR, 1.31 [95% CI, 1.17-1.47]) and household composition and disability (773 of 11 256; aPR, 1.20 [95% CI, 1.09-1.32]). Vaccination status, presence of underlying medical conditions, and respiratory symptoms partially mediated all significant associations. As social vulnerability increased, the proportion of patients receiving seasonal influenza vaccination declined (-19.4% relative change across quartiles; P < .001) as did the proportion vaccinated by October 31 (-6.8%; P < .001). No differences based on social vulnerability were found in in-hospital antiviral receipt, but early in-hospital antiviral initiation (-1.0%; P = .01) and prehospital antiviral receipt (-17.3%; P < .001) declined as social vulnerability increased.
Conclusions and relevance: In this cross-sectional study, social vulnerability was associated with a modestly increased prevalence of invasive mechanical ventilation and/or extracorporeal membrane oxygenation support among patients hospitalized with influenza. Contributing factors may have included worsened baseline respiratory health and reduced receipt of influenza prevention and prehospital or early in-hospital treatment interventions among persons residing in low socioeconomic areas.
Conflict of interest statement
Figures
References
-
- Centers for Disease Control and Prevention National Center for Immunization and Respiratory Diseases (NCIRD). About estimated flu burden. Accessed June 6, 2024. https://www.cdc.gov/flu-burden/php/about/index.html
-
- Centers for Disease Control and Prevention Agency for Toxic Substances and Disease Registry (ATSDR). CDC/ATSDR SVI fact sheet. Accessed October 21, 2022. https://www.atsdr.cdc.gov/placeandhealth/svi/fact_sheet/fact_sheet.html
-
- Centers for Disease Control and Prevention National Center for HIV Viral Hepatitis STD and TB Prevention. Health disparities in HIV, viral hepatitis, STDs, and tuberculosis. Updated September 14, 2020. Accessed January 9, 2023. https://www.cdc.gov/health-disparities-hiv-std-tb-hepatitis/index.html
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
