

Lobectomy vs Total Thyroidectomy With Ipsilateral Lateral Neck Dissection for N1b Intermediate-Risk Papillary Thyroid Carcinoma
- PMID: 39602155
- PMCID: PMC11826362
- DOI: 10.1001/jamaoto.2024.3860
Lobectomy vs Total Thyroidectomy With Ipsilateral Lateral Neck Dissection for N1b Intermediate-Risk Papillary Thyroid Carcinoma
Abstract
Importance: The management of papillary thyroid carcinoma (PTC), particularly in cases with clinically apparent lateral neck lymph node metastasis (cN1b), remains an area of debate. The surgical options for PTC, including total thyroidectomy and lobectomy, have distinct impacts on patients' outcomes and quality of life.
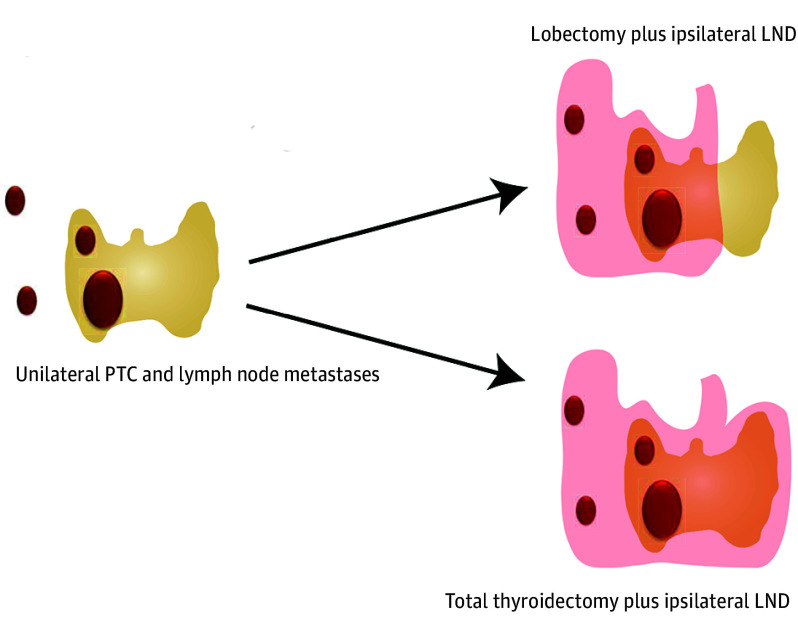
Objective: To compare survival and recurrence outcomes between patients who underwent a lobectomy plus ipsilateral lateral neck dissection (LND) and those who underwent a total thyroidectomy plus ipsilateral LND for intermediate-risk cN1b PTC with both primary tumors and lymph node metastases in the ipsilateral neck region.
Design, setting, and participants: This retrospective cohort study was conducted at Ito Hospital, Tokyo, Japan. Patients who underwent surgery for PTC between January 2005 and December 2012 were included, and those with high-risk PTCs and concurrent other thyroid cancers were excluded. Data were analyzed from April to August 2024.
Exposures: Lobectomy plus LND vs total thyroidectomy plus LND.
Main outcomes and measures: An inverse probability of treatment weighting (IPTW)-adjusted Kaplan-Meier analysis and a Cox proportional hazards regression analysis were performed to compare the patients' overall survival, recurrence-free survival (RFS), and modified RFS (which considered the potential need for a future contralateral lobectomy).
Results: Of 401 included patients, 317 (79.1%) were female, and the median (IQR) age was 47 (36-59) years. A total of 157 patients underwent lobectomy plus ipsilateral LND and 244 underwent total thyroidectomy plus ipsilateral LND. The median (IQR) follow-up time was 13.0 (11.2-15.0) years. The IPTW-adjusted overall survival rates at 5, 10, and 15 years were 98.0% (95% CI, 93.9-99.3), 97.5% (95% CI, 93.2-99.1), and 96.8% (95% CI, 92.2-98.7), respectively, for the lobectomy group vs 99.4% (95% CI, 97.0-99.9), 97.4% (95% CI, 94.4-98.8), and 96.9% (95% CI, 93.3-98.5), respectively, for the total thyroidectomy group (hazard ratio [HR], 1.10; 95% CI, 0.35-3.47). The IPTW-adjusted RFS rates at 5, 10, and 15 years were 93.8% (95% CI, 88.5-96.7), 88.4% (95% CI, 82.0-92.6), and 84.1% (95% CI, 76.8-89.3), respectively, for the lobectomy group vs 95.4% (95% CI, 91.8-97.4), 92.9% (95% CI, 88.8-95.5), and 87.8% (95% CI, 80.8-92.4), respectively, for the total thyroidectomy group (HR, 1.41; 95% CI, 0.79-2.54). The IPTW-adjusted modified RFS rates at 5, 10, and 15 years were 96.7% (95% CI, 92.2-98.6), 93.8% (95% CI, 88.5-96.7), and 88.9% (95% CI, 82.4-93.1), respectively, for the lobectomy group vs 95.4% (95% CI, 91.8-97.4), 92.9% (95% CI, 88.8-95.5), and 87.8% (95% CI, 80.8-92.4), respectively, for the total thyroidectomy group (HR, 0.93; 95% CI, 0.49-1.76).
Conclusions and relevance: In this study, for these selected intermediate-risk cN1b PTC cases, total thyroidectomy and lobectomy provided comparable outcomes in terms of prognosis and recurrence. These data may help inform future guideline revisions and support joint decision-making between patients and their clinicians.
Conflict of interest statement
Figures


References
-
- Haugen BR, Alexander EK, Bible KC, et al. . 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26(1):1-133. doi:10.1089/thy.2015.0020 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
