

Ravulizumab and Efgartigimod in Myasthenia Gravis: A Real-World Study
- PMID: 39602677
- PMCID: PMC11604103
- DOI: 10.1212/NXI.0000000000200331
Ravulizumab and Efgartigimod in Myasthenia Gravis: A Real-World Study
Abstract
Background and objectives: Biologics that target pathogenic antibodies (Abs) and their effector functions such as the complement inhibitor ravulizumab and the neonatal Fc receptor agonist efgartigimod have recently been approved for the treatment of acetylcholine receptor (AChR)-Ab-positive myasthenia gravis (MG), but comparative studies are lacking.
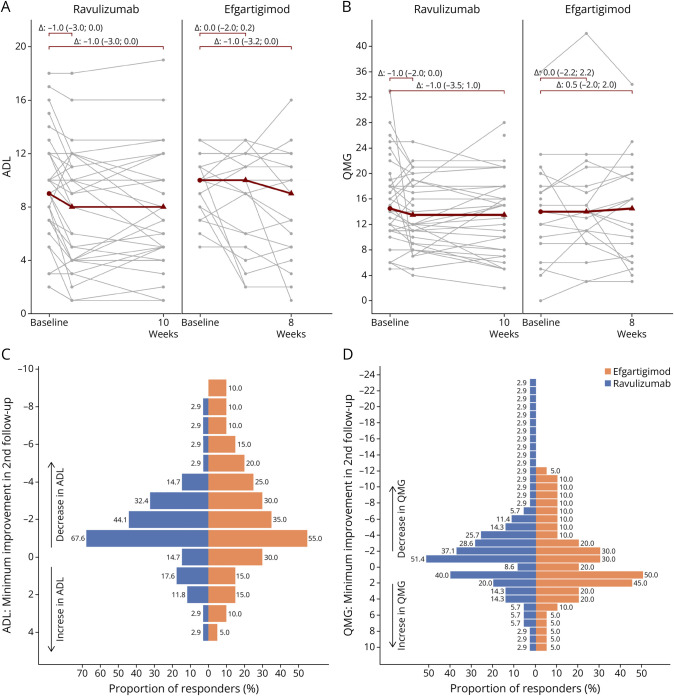
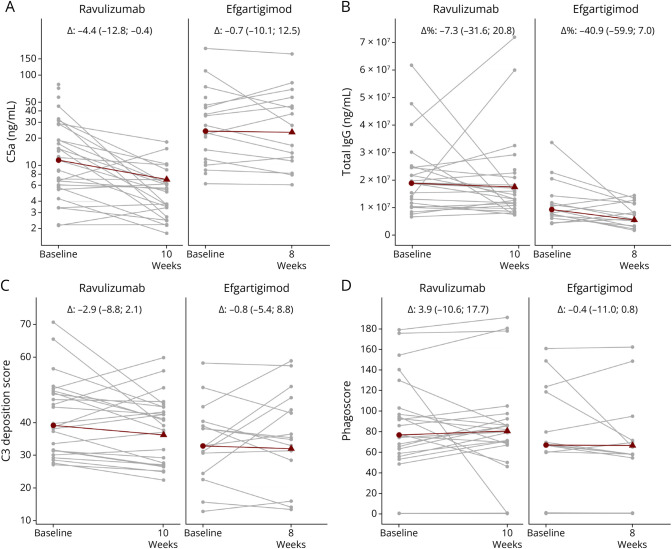
Methods: In a prospective, exploratory real-world study, we assessed clinical efficacy, safety, and biological effects of ravulizumab and efgartigimod treatment initiation. Myasthenia Gravis-Activities of Daily Living and Quantitative Myasthenia Gravis scores were used as clinical endpoints. Ab effector functions were determined by AChR-Ab-dependent complement activation and phagocytosis assays and systemic complement activation profiling.
Results: We observed similar moderate short-term efficacy of ravulizumab and efgartigimod in achieving clinical improvement. Ravulizumab reduced systemic terminal complement activation, but neither treatment showed significant effects on complement pathways proximal to C5 or functional capacities of AChR-Abs. Both treatment modalities were well tolerated with no serious adverse events reported.
Discussion: Clinical benefits obtained with ravulizumab and efgartigimod can be remarkably heterogeneous in daily clinical practice. Neither treatment relevantly changed effector functions of pathogenic AChR-Abs, supporting the concept that durable disease control in MG requires continuous administration of both fast-acting agents.
Classification of evidence: This study provides Class III evidence that in AChR-Ab-positive patients with generalized MG, ravulizumab and efgartigimod provide comparable modest improvement in MG functional scales.
Conflict of interest statement
F. Stascheit received travel/accommodation/meeting expenses from Alexion Pharmaceuticals and argnx and received speaking honoria and honoria for attendance at advisory boards from Alexion Pharmaceuticals, argnx and UCB pharma; A. Aigner and M. Behrens reports no conflict of interests; C.W. Keller received travel, accommodation and meeting expenses from Alexion and UCB; L. Klotz received speaking honoraria and travel/meeting expenses from Argenx, Bayer, Biogen, Bristol-Myers Squibb, Genzyme, Grifols, Merck Serono, Novartis, Roche, Santhera and Teva. She participated in Advisory Boards for Alexion, Biogen, Bristol-Myers Squibb, Genzyme, Horizon, Janssen, Merck Serono, Novartis, Roche, Sandoz and Viatris; S. Lehnerer has received speakers honoraria from Alexion, argenx, Hormosan and UCB, honoraria for attendance at advisory boards from Alexion, argenx, Biogen, UCB and Roche, travel/accommodation/meeting expenses from Alexion Pharmaceuticals and argnx and research funding from Hormosan, Alexion, UCB and argnx; M. Stein has received speaking honoria and honoria for attendance at advisory boards from Argenx and Alexion Pharmaceuticals; M. Herdick has received speaker's honaria from argenx; P. Doksani and L. Gerischer reports no conflict of interest; S. Hoffmann has received speakers' honoraria from Alexion, argenx, UCB, Grifols and Roche, honoraria for attendance at advisory boards from Alexion, argenx and Roche and research funding from argenx and Janssen. S. Hoffmann is member of the medical advisory board of the German Myasthenia Society, DMG. K. Lazaridis reports no conflict of interest; J. Tzartos reports speaking honoria from Astra Zeneca and Medison Pharma; H. Wiendl received speaker honoraria from Alexion, Biogen, Bristol Myers Squibb, Genzyme, Merck, Neurodiem, Novartis, Ology, Roche, TEVA, and WebMD Global. He received honoraria for consulting services from Abbvie, Actelion, Argenx, BD, Bristol Myers Squibb, EMD Serono, Fondazione Cariplo, Gossamer Bio, Idorsia, Immunic, Immunovant, INmune Bio_Syneos Health, Janssen, Merck, NexGen, Novartis, Roche, Sanofi, Swiss MS Society, UCB and Worldwide Clinical Trials. His research is supported by the German Myasthenia Gravis Society; A. Meisel received speaker or consultancy honoraria or financial research support (paid to his institution) from Alexion Pharmaceuticals, argenx, Axunio, Destin, Grifols, Hormosan Pharma, Janssen, Merck, Octapharma, UCB, and Xcenda. He serves as medical advisory board chairman of the German Myasthenia Gravis Society; J.D. Lünemann has received speaker fees, research support, travel support, and/or served on advisory boards by Abbvie, Alexion, Argenx, Biogen, Merck, Moderna, Novartis, Roche, Sanofi and Takeda, and is member of the medical advisory board of the German Myasthenia Gravis Society. Go to
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous