

Development and Validation of a Prediction Model Using Sella Magnetic Resonance Imaging-Based Radiomics and Clinical Parameters for the Diagnosis of Growth Hormone Deficiency and Idiopathic Short Stature: Cross-Sectional, Multicenter Study
- PMID: 39602803
- PMCID: PMC11635315
- DOI: 10.2196/54641
Development and Validation of a Prediction Model Using Sella Magnetic Resonance Imaging-Based Radiomics and Clinical Parameters for the Diagnosis of Growth Hormone Deficiency and Idiopathic Short Stature: Cross-Sectional, Multicenter Study
Abstract
Background: Growth hormone deficiency (GHD) and idiopathic short stature (ISS) are the major etiologies of short stature in children. For the diagnosis of GHD and ISS, meticulous evaluations are required, including growth hormone provocation tests, which are invasive and burdensome for children. Additionally, sella magnetic resonance imaging (MRI) is necessary for assessing etiologies of GHD, which cannot evaluate hormonal secretion. Recently, radiomics has emerged as a revolutionary technique that uses mathematical algorithms to extract various features for the quantitative analysis of medical images.
Objective: This study aimed to develop a machine learning-based model using sella MRI-based radiomics and clinical parameters to diagnose GHD and ISS.
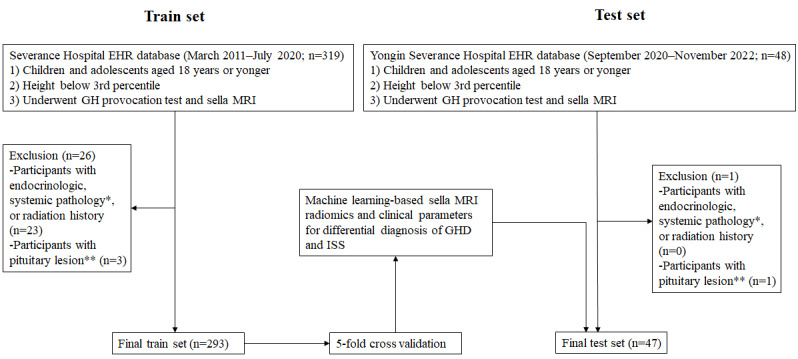
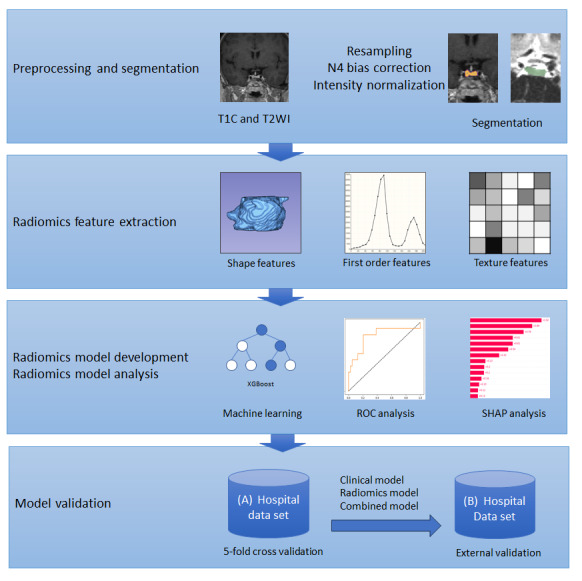
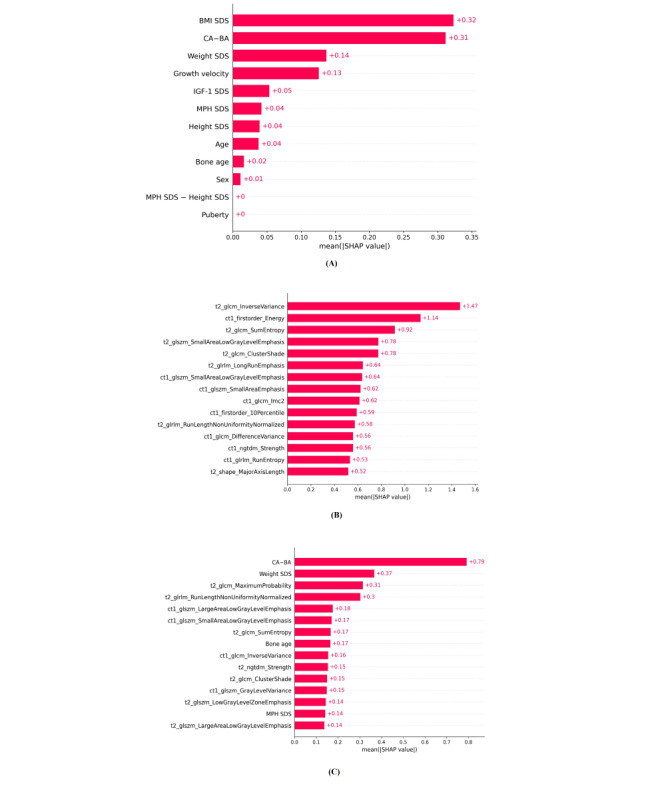
Methods: A total of 293 children with short stature who underwent sella MRI and growth hormone provocation tests were included in the training set, and 47 children who met the same inclusion criteria were enrolled in the test set from different hospitals for this study. A total of 186 radiomic features were extracted from the pituitary glands using a semiautomatic segmentation process for both the T2-weighted and contrast-enhanced T1-weighted image. The clinical parameters included auxological data, insulin-like growth factor-I, and bone age. The extreme gradient boosting algorithm was used to train the prediction models. Internal validation was conducted using 5-fold cross-validation on the training set, and external validation was conducted on the test set. Model performance was assessed by plotting the area under the receiver operating characteristic curve. The mean absolute Shapley values were computed to quantify the impact of each parameter.
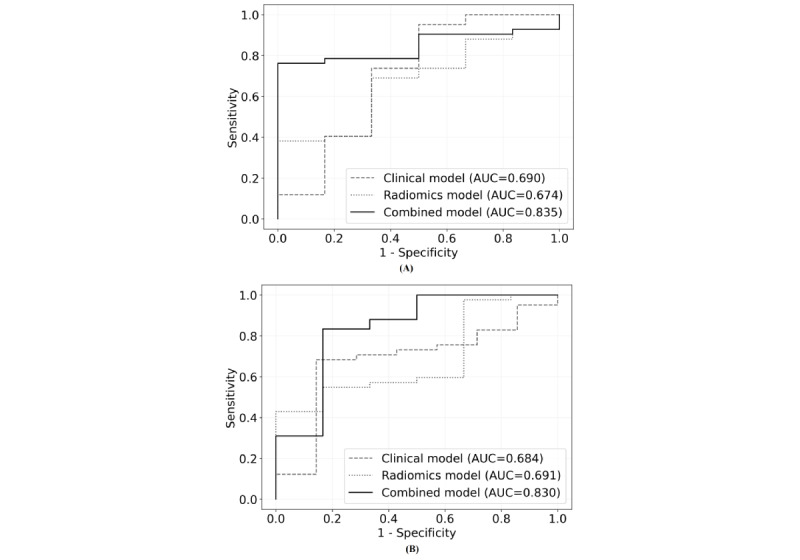
Results: The area under the receiver operating characteristic curves (95% CIs) of the clinical, radiomics, and combined models were 0.684 (0.590-0.778), 0.691 (0.620-0.762), and 0.830 (0.741-0.919), respectively, in the external validation. Among the clinical parameters, the major contributing factors to prediction were BMI SD score (SDS), chronological age-bone age, weight SDS, growth velocity, and insulin-like growth factor-I SDS in the clinical model. In the combined model, radiomic features including maximum probability from a T2-weighted image and run length nonuniformity normalized from a T2-weighted image added incremental value to the prediction (combined model vs clinical model, P=.03; combined model vs radiomics model, P=.02). The code for our model is available in a public repository on GitHub.
Conclusions: Our model combining both radiomics and clinical parameters can accurately predict GHD from ISS, which was also proven in the external validation. These findings highlight the potential of machine learning-based models using radiomics and clinical parameters for diagnosing GHD and ISS.
Keywords: MRI; adolescent; child; dwarfism; idiopathic short stature; machine learning; magnetic resonance imaging; pituitary.
©Kyungchul Song, Taehoon Ko, Hyun Wook Chae, Jun Suk Oh, Ho-Seong Kim, Hyun Joo Shin, Jeong-Ho Kim, Ji-Hoon Na, Chae Jung Park, Beomseok Sohn. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 27.11.2024.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Song KC, Jin SL, Kwon AR, Chae HW, Ahn JM, Kim DH, Kim H. Etiologies and characteristics of children with chief complaint of short stature. Ann Pediatr Endocrinol Metab. 2015 Mar;20(1):34–9. doi: 10.6065/apem.2015.20.1.34. https://europepmc.org/abstract/MED/25883925 - DOI - PMC - PubMed
-
- Song K, Lee J, Lee S, Jeon S, Lee HS, Kim H, Chae HW. Height and subjective body image are associated with suicide ideation among Korean adolescents. Front Psychiatry. 2023;14:1172940. doi: 10.3389/fpsyt.2023.1172940. https://europepmc.org/abstract/MED/37377472 - DOI - PMC - PubMed
-
- Park SH, Lee YJ, Cheon J, Shin CH, Jung HW, Lee YA. The effect of hypothalamic involvement and growth hormone treatment on cardiovascular risk factors during the transition period in patients with childhood-onset craniopharyngioma. Ann Pediatr Endocrinol Metab. 2023;28(2):107–115. doi: 10.6065/apem.2244046.023. https://europepmc.org/abstract/MED/35798299 apem.2244046.023 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
