

Clinical comparison and genetic analysis in pheochromocytoma with primary aldosteronism
- PMID: 39603607
- PMCID: PMC11850107
- DOI: 10.1507/endocrj.EJ24-0150
Clinical comparison and genetic analysis in pheochromocytoma with primary aldosteronism
Abstract
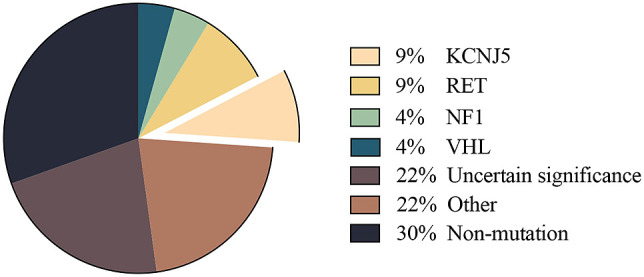
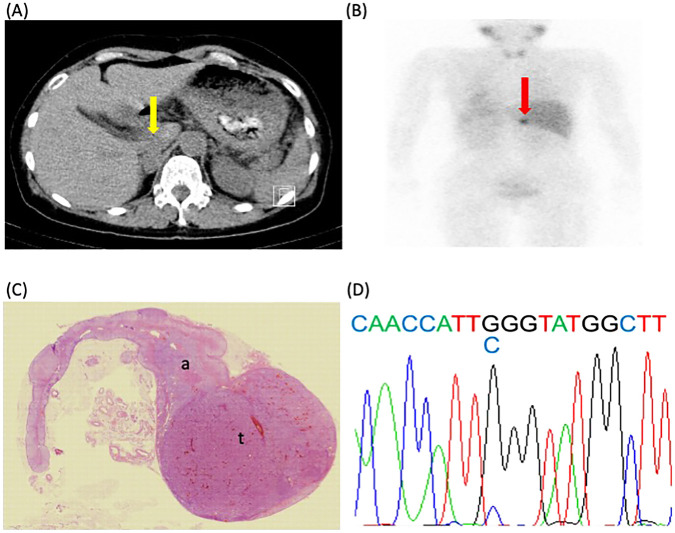
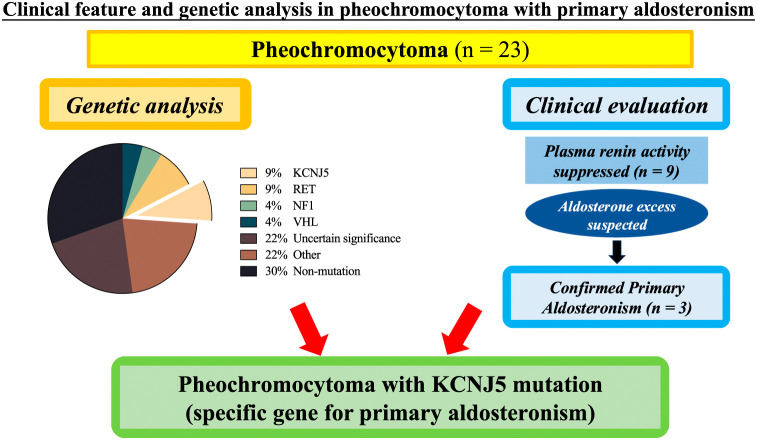
Pheochromocytoma is a rare form of adrenal hypertension. This study aimed to investigate the clinical characteristics and associated genetic mutations in patients with pheochromocytoma and primary aldosteronism. We retrospectively analyzed data from 23 patients with pheochromocytoma diagnosed and treated between 2011 and 2022. Three cases were complicated by primary aldosteronism. Compared to 15 other patients without primary aldosteronism complications, these three patients had a greater suppression of plasma renin activity (0.2 vs. 2.3 ng/mL/h, p < 0.01) and a higher aldosterone-to-renin ratio (p < 0.01). No significant differences were found in blood pressure, serum potassium levels, or plasma aldosterone concentrations between the two groups. In genetic analysis, among the three patients with pheochromocytoma and primary aldosteronism, two had a KCNJ5 (G151R) mutation in the pheochromocytoma tumor tissues. However, no CYP11B2- or CYP11B1-positive cells were detected via immunostaining in the pheochromocytoma tissues of these three patients. To our knowledge, this is the first study to reveal the presence of the KCNJ5 mutation, commonly considered specific to primary aldosteronism, in pheochromocytoma cases clinically complicated by primary aldosteronism. The findings suggest that patients with pheochromocytoma and suppressed plasma renin activity should be assessed for primary aldosteronism.
Keywords: KCNJ5; Next-generation sequencing; Pheochromocytoma; Primary aldosteronism.
Conflict of interest statement
None of the authors have any potential conflicts of interest associated with this research.
Figures

References
-
- Umemura S, Arima H, Arima S, Asayama K, Dohi Y, et al. (2019) The Japanese Society of Hypertension guidelines for the management of hypertension (JSH 2019). Hypertens Res 42: 1235–1481. - PubMed
-
- Lenders JWM, Eisenhofer G, Mannelli M, Pacak K (2005) Phaeochromocytoma. Lancet 366: 665–675. - PubMed
-
- Anderson GH Jr, Blakeman N, Streeten DH (1994) The effect of age on prevalence of secondary forms of hypertension in 4,429 consecutively referred patients. J Hypertens 12: 609–615. - PubMed
-
- Omura M, Saito J, Yamaguchi K, Kakuta Y, Nishikawa T (2004) Prospective study on the prevalence of secondary hypertension among hypertensive patients visiting a general outpatient clinic in Japan. Hypertens Res 27: 193–202. - PubMed