

Risk Factors, Treatments, and Outcomes of Adults Aged <55 Years With Acute Ischemic Stroke With Undetermined Versus Determined Pathogenesis: A Nationwide Swiss Cohort Study
- PMID: 39604021
- PMCID: PMC11681592
- DOI: 10.1161/JAHA.124.036761
Risk Factors, Treatments, and Outcomes of Adults Aged <55 Years With Acute Ischemic Stroke With Undetermined Versus Determined Pathogenesis: A Nationwide Swiss Cohort Study
Abstract
Background: The rising prevalence of acute ischemic stroke (AIS) in young adults, particularly with undetermined pathogenesis, is a growing concern. This study assessed risk factors, treatments, and outcomes between young AIS patients with undetermined and determined pathogeneses.
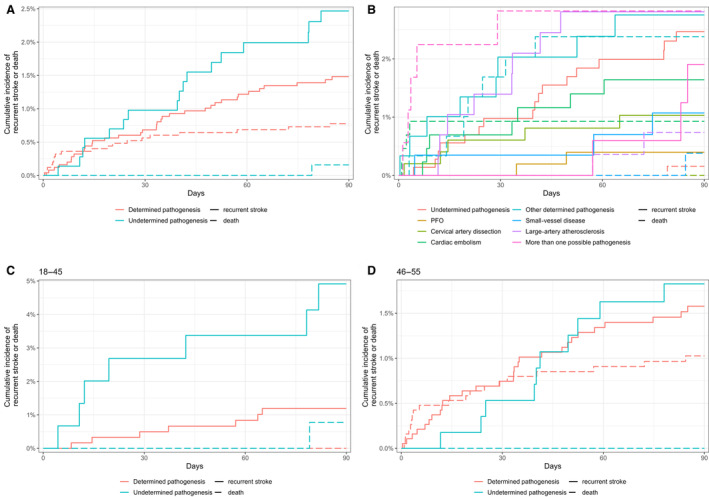
Methods and results: This was a retrospective cohort study including AIS patients aged 18 to 55 years in Switzerland, treated between 2014 and 2022. Stroke pathogeneses were classified using a modified TOAST (Trial of ORG 10172 in Acute Stroke Treatment) classification, with undetermined pathogenesis defined as no identified cause (including patent foramen ovale and cervical artery dissection). We examined vascular risk factors, acute treatments, 3-month functional outcomes, and AIS recurrence within 3 months using logistic regression and Fine-Gray proportional hazards models. Of 3995 patients, 863 (22%) had undetermined pathogenesis. Compared with patients with determined pathogenesis, those with undetermined pathogenesis had a higher prevalence of dyslipidemia (54% versus 59%, P=0.007) and smoking (37% versus 43%, P=0.001), and were more likely to receive intravenous thrombolysis (27% versus 31%, P=0.046). Despite higher 3-month AIS recurrence risk for the undetermined group (adjusted hazard ratio, 1.72 [95% CI, 1.01-2.94]), favorable functional outcomes at 3 months were more frequent (modified Rankin Scale score, 0-2: 90% versus 87%, P=0.033). Patients aged 46 to 55 years with undetermined pathogenesis had better outcomes than those with determined pathogenesis (modified Rankin Scale score, 0-1: 70% versus 64%, P=0.013; modified Rankin Scale score, 0-2: 89% versus 85%, P=0.023), while those aged 18 to 45 years showed higher recurrence rates (4.5% versus 1.8%, P<0.05) but similar functional outcomes.
Conclusions: Young adults with AIS exhibit a considerable vascular risk burden. Those with undetermined pathogenesis displayed age-related outcome disparities, with better short-term outcomes in older and higher recurrence rates in younger patients.
Keywords: ischemic stroke; undetermined pathogenesis; vascular risk factors; young.
Conflict of interest statement
None.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
