

Assessment of circulating tumor DNA in patients with locally advanced rectal cancer treated with neoadjuvant therapy
- PMID: 39604448
- PMCID: PMC11603181
- DOI: 10.1038/s41598-024-80855-8
Assessment of circulating tumor DNA in patients with locally advanced rectal cancer treated with neoadjuvant therapy
Abstract
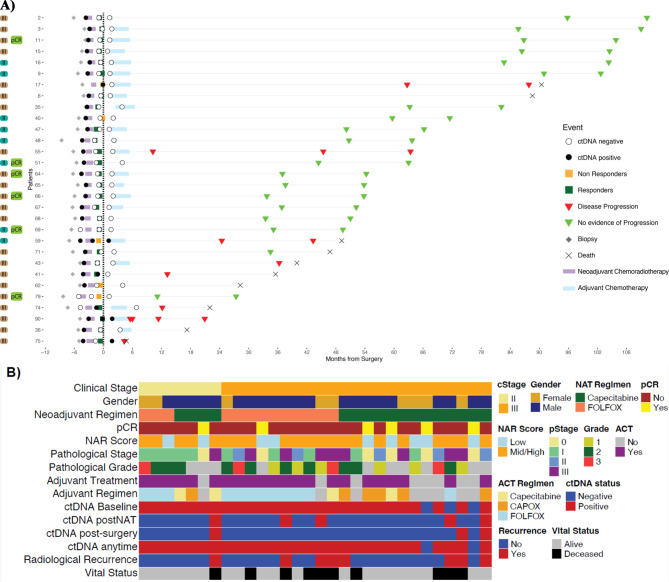
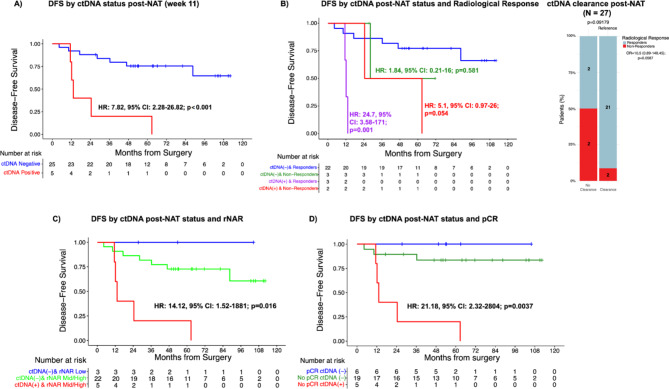
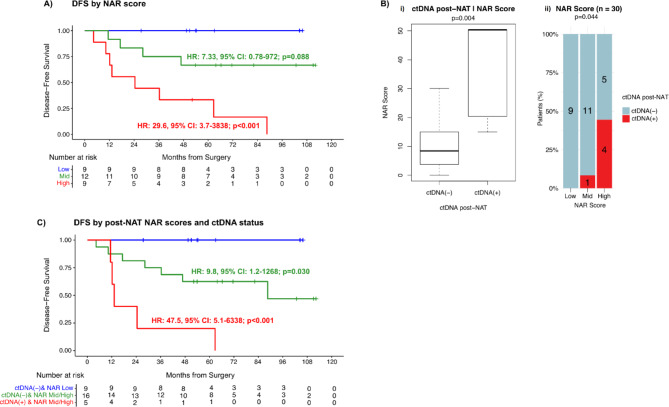
Post-neoadjuvant therapy (post-NAT) and post-surgical circulating tumor DNA (ctDNA) risk stratification may enhance the management of patients with locally advanced rectal cancer (LARC). In this study, we assessed the prognostic value of ctDNA-based MRD detection in LARC patients using a personalized, tumor-informed ctDNA assay. Plasma samples from LARC patients (N = 30) were analyzed retrospectively using the Signatera™ assay. The neoadjuvant rectal (NAR) score was calculated and compared to ctDNA status to predict recurrence risk and survival outcomes. ctDNA-positive patients post-NAT and post-surgery had worse Disease Free Survival (DFS) (HR: 7.82; p = 0.001, HR: 19.65; p = 0.001) when compared to ctDNA-negative patients. In the post-NAT setting, patients who responded to NAT had superior DFS compared to patients who did not clear their ctDNA or showed no radiological response (HR: 24.7, p = 0.001 and HR: 5.1, p = 0.054, respectively). When ctDNA status is used alongside the NAR score in the post-NAT setting, patients who were ctDNA-positive with an intermediate or high NAR score showed significantly worse DFS (HR: 47.5, p < 0.001) compared to ctDNA-negative patients with either a low or intermediate/high NAR score (HR: 9.8, p = 0.0301). Post-NAT ctDNA status, whether used alone or in combination with the NAR score, may predict NAT response, and improve risk stratification.
Keywords: Biomarker; Circulating tumor DNA; Locally advanced rectal cancer; NAR score; Neoadjuvant therapy.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures

References
-
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for rectal Cancer Version 1.2024. © National Comprehensive Cancer Network, Inc. (2024).
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
