

Tailoring glioblastoma treatment based on longitudinal analysis of post-surgical tumor microenvironment
- PMID: 39605004
- PMCID: PMC11603899
- DOI: 10.1186/s13046-024-03231-4
Tailoring glioblastoma treatment based on longitudinal analysis of post-surgical tumor microenvironment
Abstract
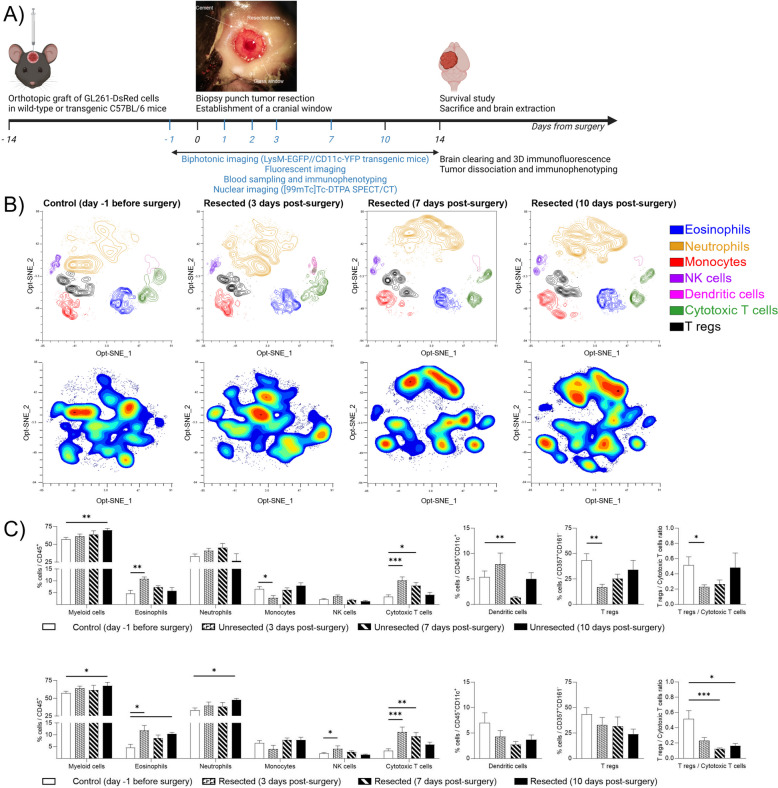
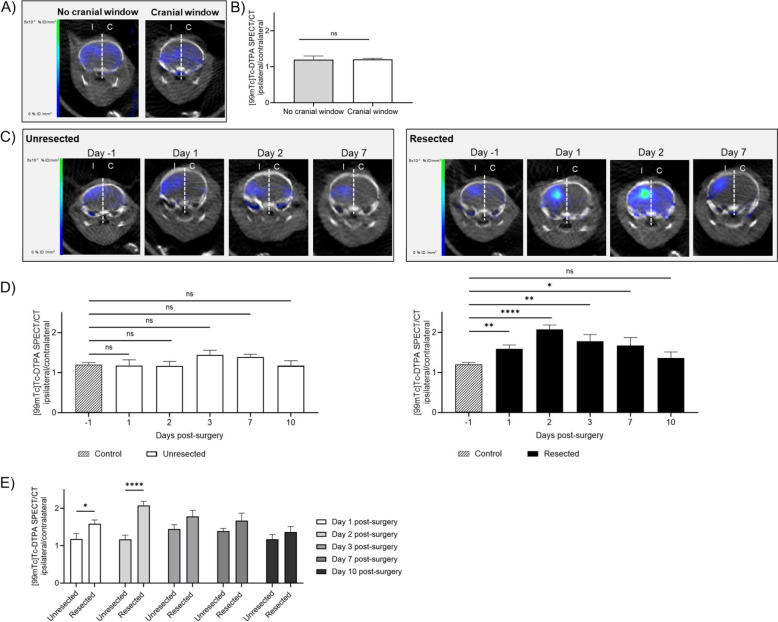
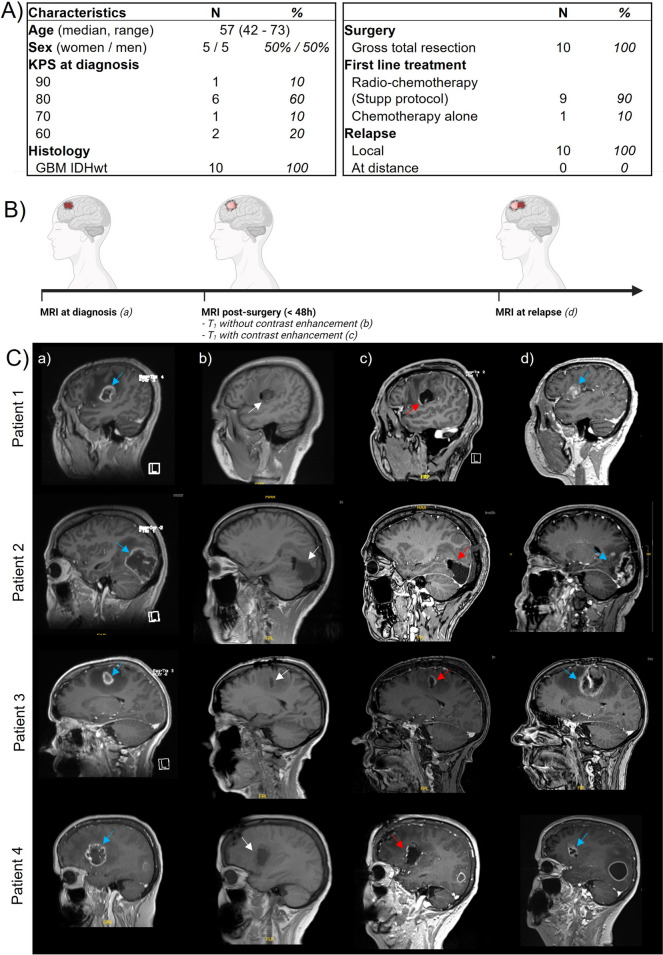
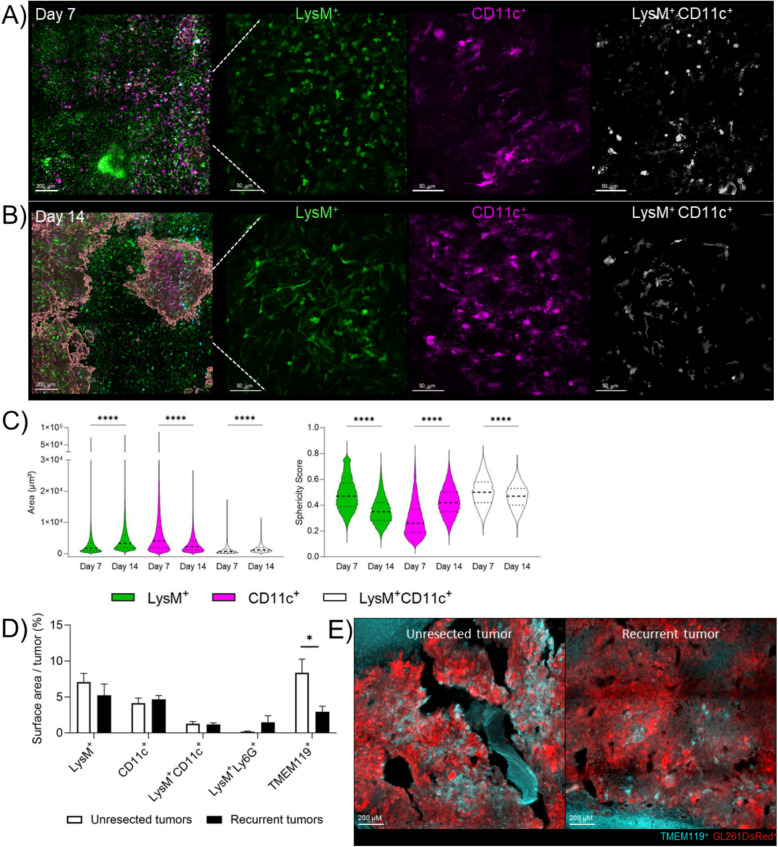
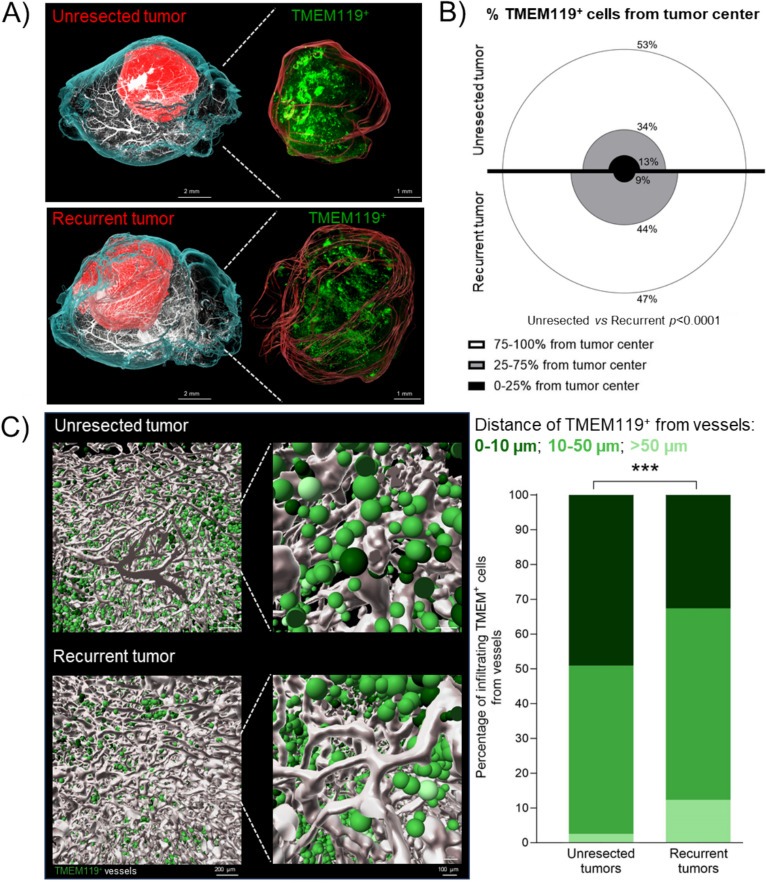
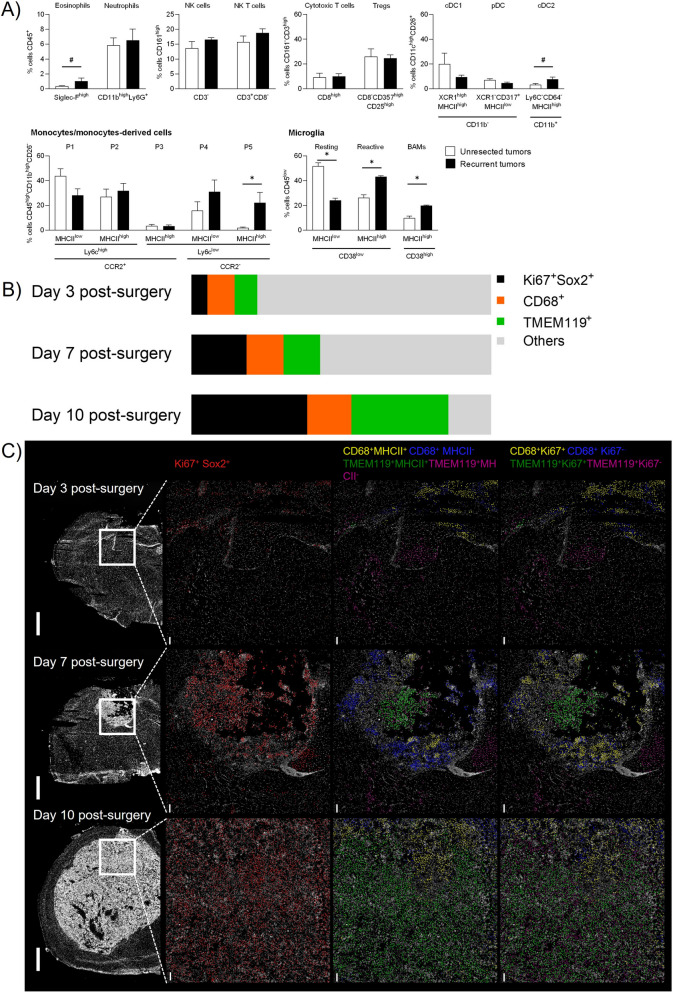
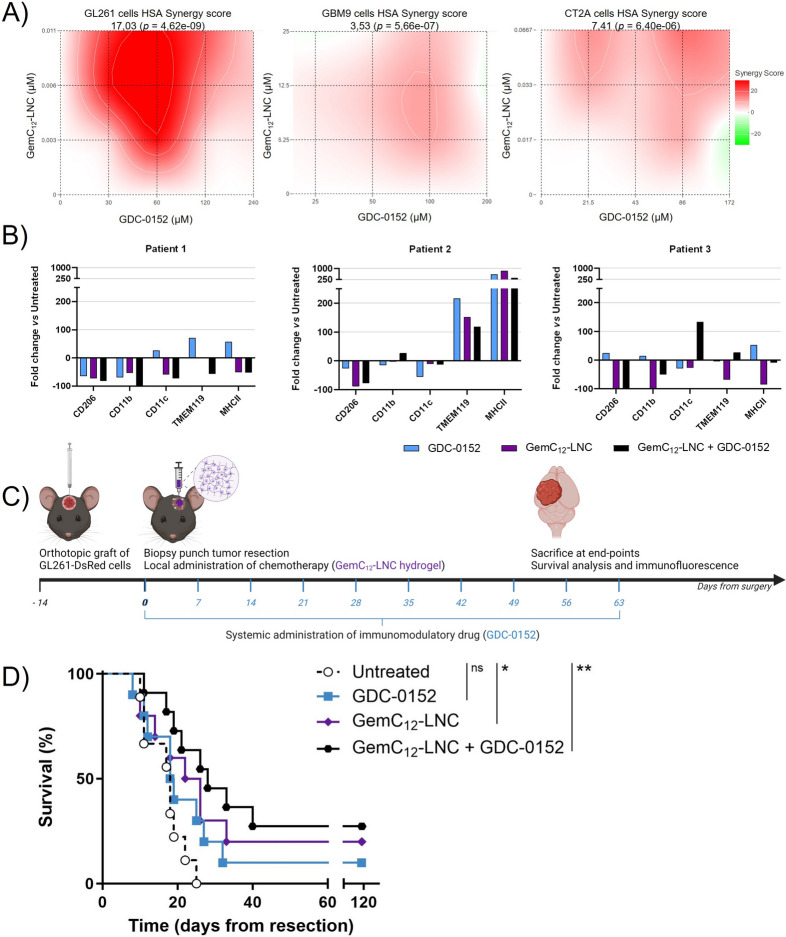
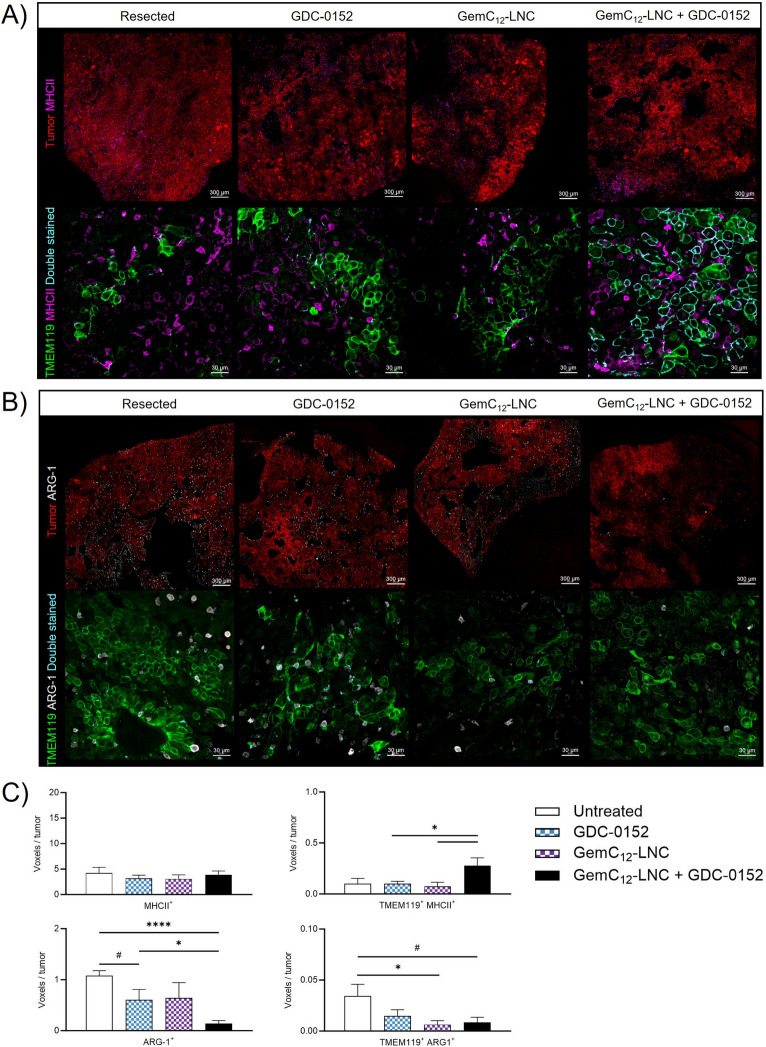
Glioblastoma (GBM), an incurable primary brain tumor, typically requires surgical intervention followed by chemoradiation; however, recurrences remain fatal. Our previous work demonstrated that a nanomedicine hydrogel (GemC12-LNC) delays recurrence when administered post-surgery. However, tumor debulking also triggers time-dependent immune reactions that promote recurrence at the resection cavity borders. We hypothesized that combining the hydrogel with an immunomodulatory drug could enhance therapeutic outcomes. A thorough characterization of the post-surgical microenvironment (SMe) is crucial to guide combinatorial approaches.In this study, we performed cellular resolution imaging, flow cytometry and spatial hyperplexed immunofluorescence imaging to characterize the SMe in a syngeneic mouse model of tumor resection. Owing to our dynamic approach, we observed transient opening of the blood-brain barrier (BBB) during the first week after surgery. BBB permeability post-surgery was also confirmed in GBM patients. In our murine model, we also observed changes in immune cell morphology and spatial location post-surgery over time in resected animals as well as the accumulation of reactive microglia and anti-inflammatory macrophages in recurrences compared to unresected tumors since the first steps of recurrence growth. Therefore we investigated whether starting a systemic treatment with the SMAC mimetic small molecule (GDC-0152) directly after surgery would be beneficial for enhancing microglial anti-tumoral activity and decreasing the number of anti-inflammatory macrophages around the GemC12-LNC hydrogel-loaded tumor cavity. The immunomodulatory effects of this drug combination was firstly shown in patient-derived tumoroids. Its efficacy was confirmed in vivo by survival analysis and correlated with reversal of the immune profile as well as delayed tumor recurrence.This comprehensive study identified critical time frames and immune cellular targets within the SMe, aiding in the rational design of combination therapies to delay recurrence onset. Our findings suggest that post-surgical systemic injection of GDC-0152 in combination with GemC12-LNC local treatment is a promising and innovative approach for managing GBM recurrence, with potential for future translation to human patient.
Keywords: Brain tumor surgery; Drug Delivery; Glioblastoma; Neuro-oncology; Targeted therapy; Tumor microenvironment.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All patient data were obtained according to a protocol approved by the local institutional review board and ethical committee (PADS 20–343). The present study was conducted in accordance with the declaration of Helsinki. The in vivo experiments reported in this work have been approved by the institution’s Animal Care and Use Committee (CE71, Aix-Marseille Université, reference n° 22185) and performed following the French national regulation guidelines in accordance with EU Directive 2010/63/EU. Competing interests: The authors report no competing interests within this study.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
