

Metastatic recurrence in women diagnosed with non-metastatic breast cancer: a systematic review and meta-analysis
- PMID: 39605105
- PMCID: PMC11603627
- DOI: 10.1186/s13058-024-01881-y
Metastatic recurrence in women diagnosed with non-metastatic breast cancer: a systematic review and meta-analysis
Abstract
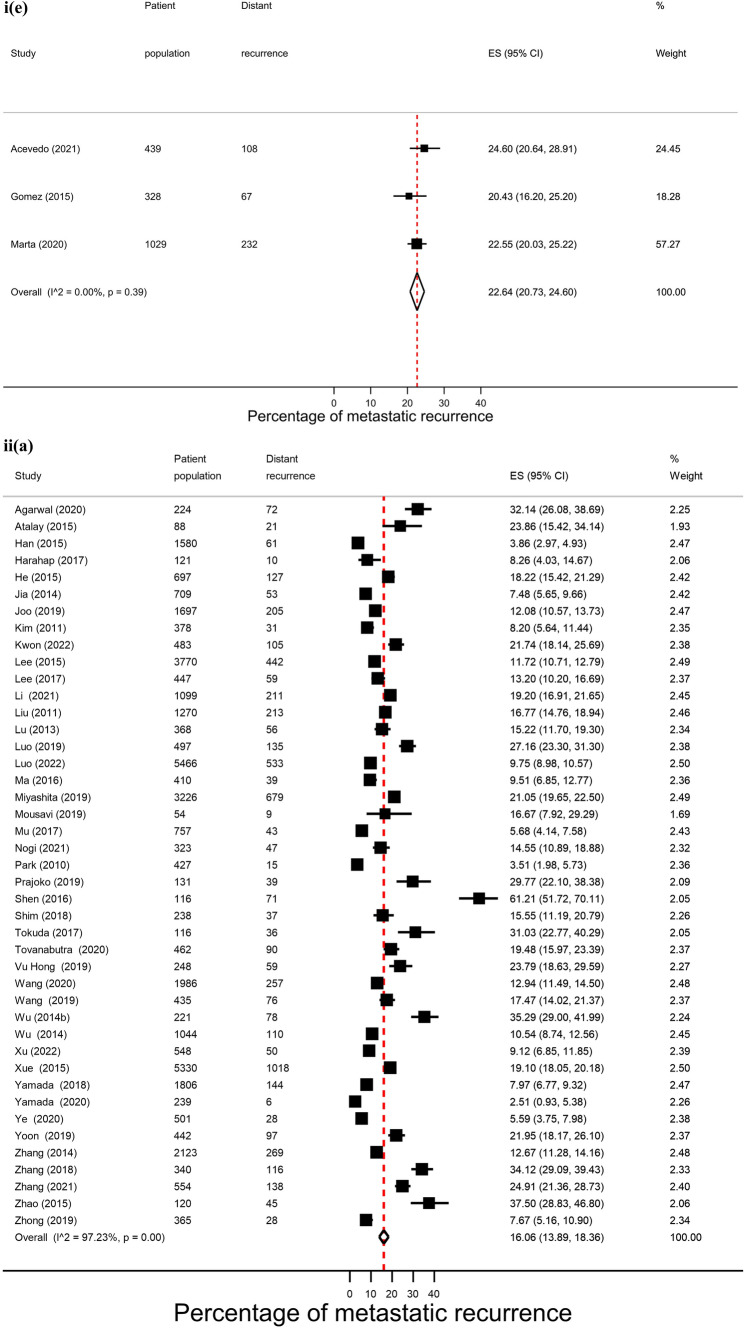
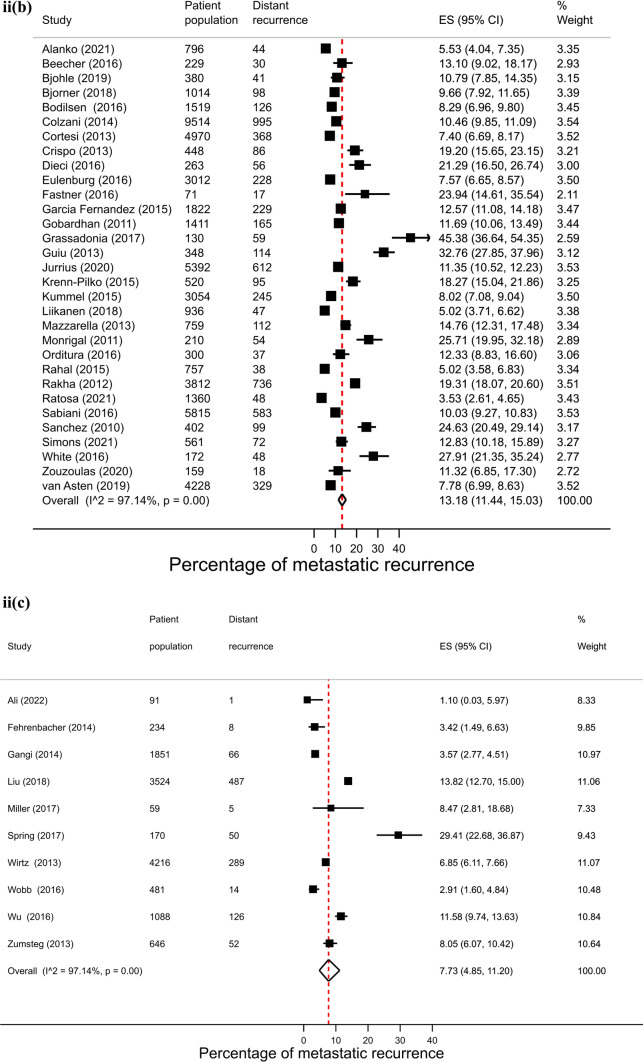
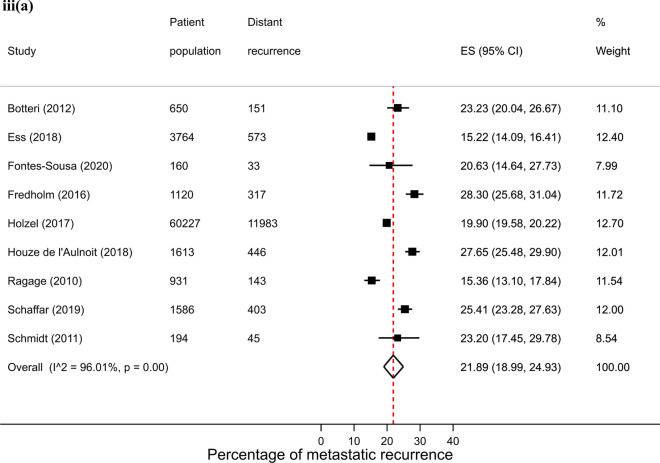
Background: To assess proportions of metastatic recurrence in women initially diagnosed with non-metastatic breast cancer by stage at diagnosis, breast cancer subtype, calendar period and age.
Methods: A systematic search of MEDLINE and Web of Science databases (January 2010-12 May 2022) was conducted. Studies reporting the proportion of distant metastatic recurrence in women with non-metastatic breast cancer were identified and outcomes and characteristics were extracted. Risk of bias was assessed independently by two reviewers. Random-effects meta-analyses of proportions were used to calculate pooled estimates and 95% confidence intervals (CIs).
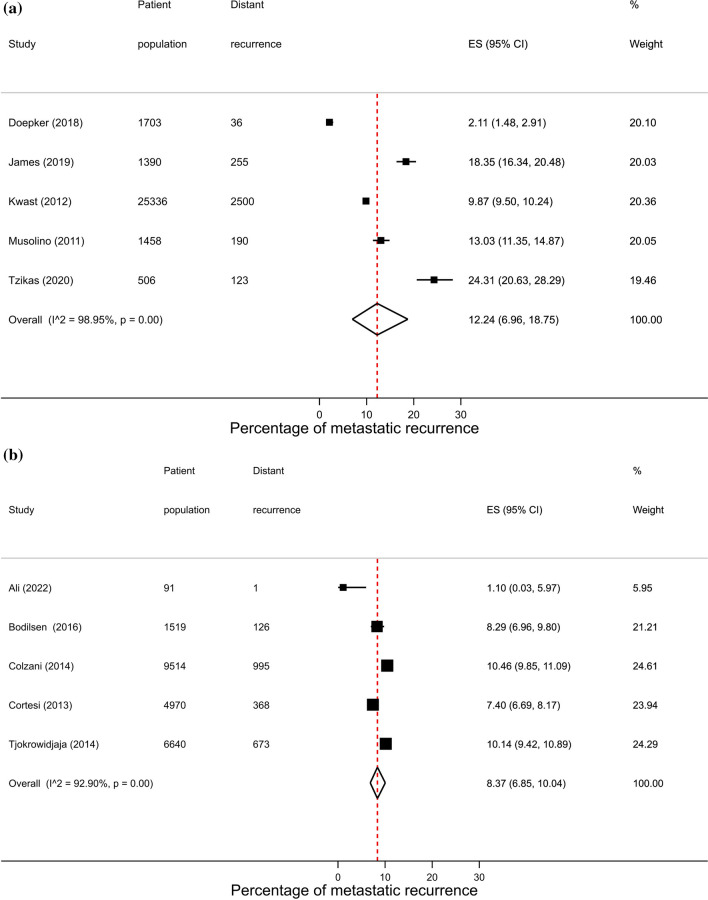
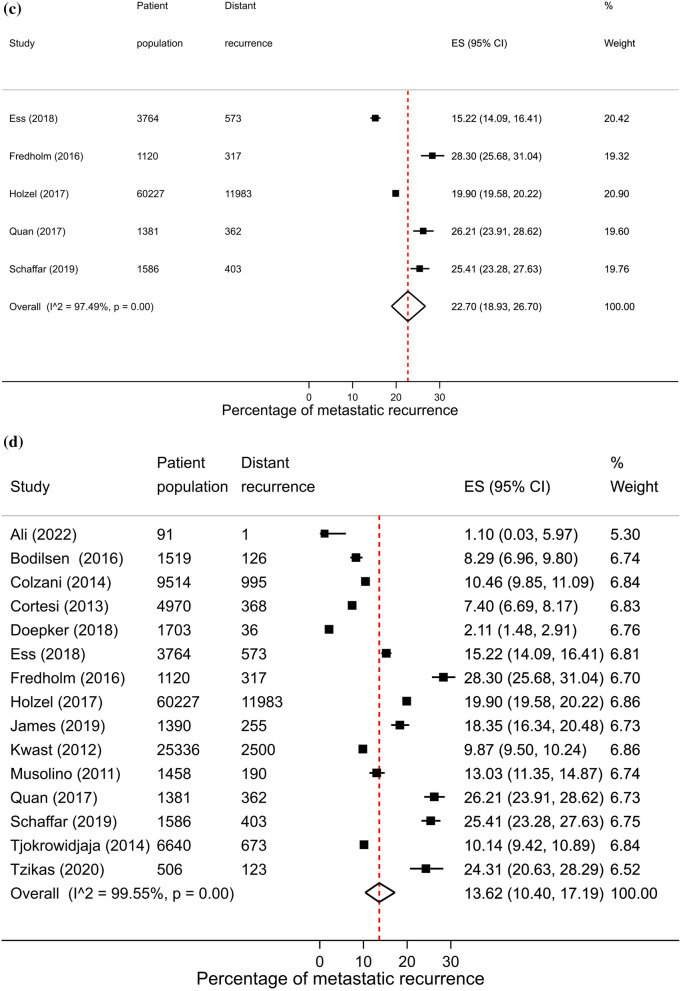
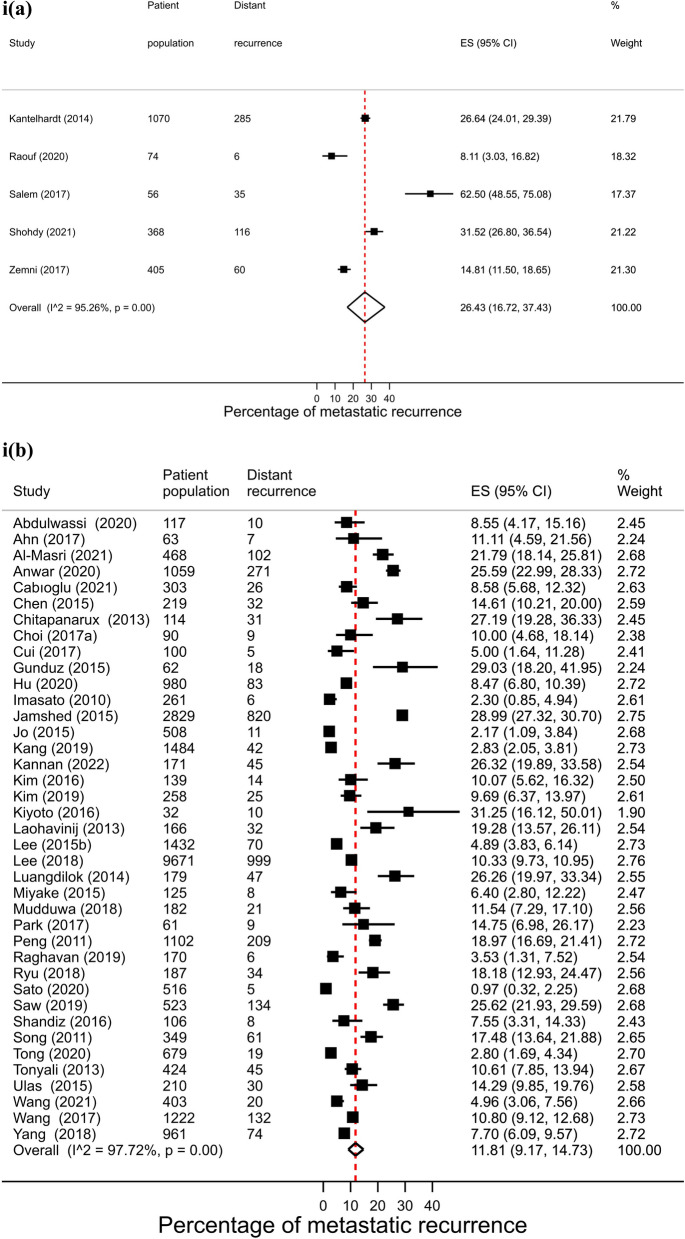
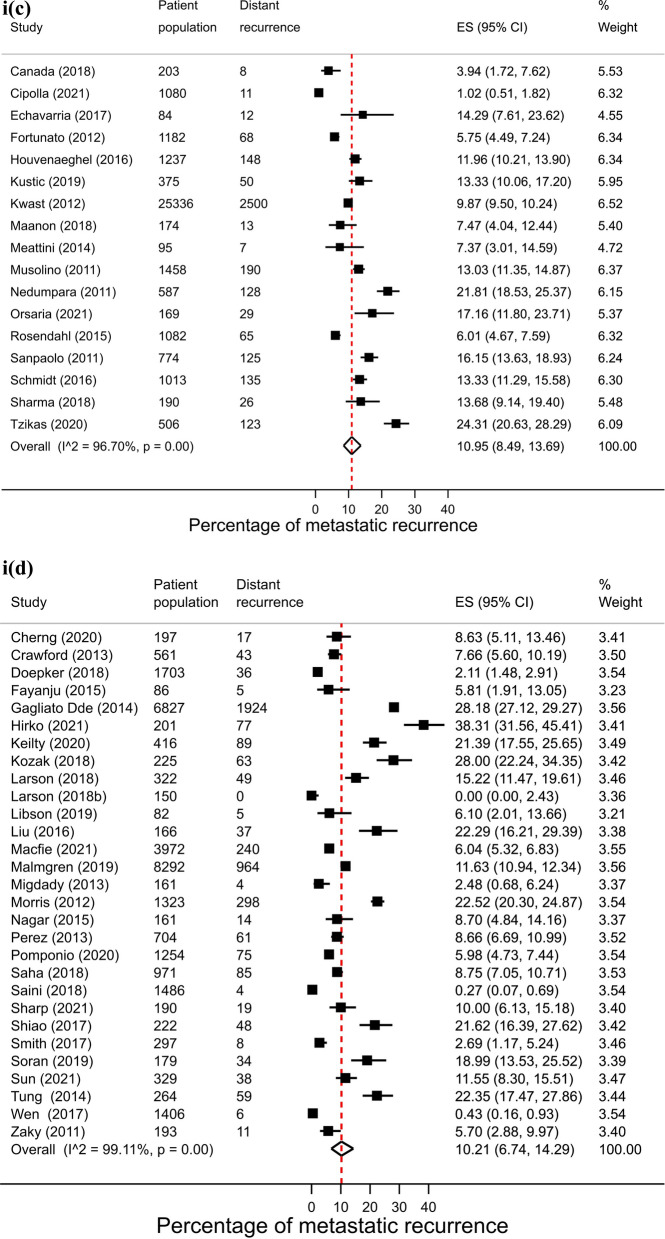
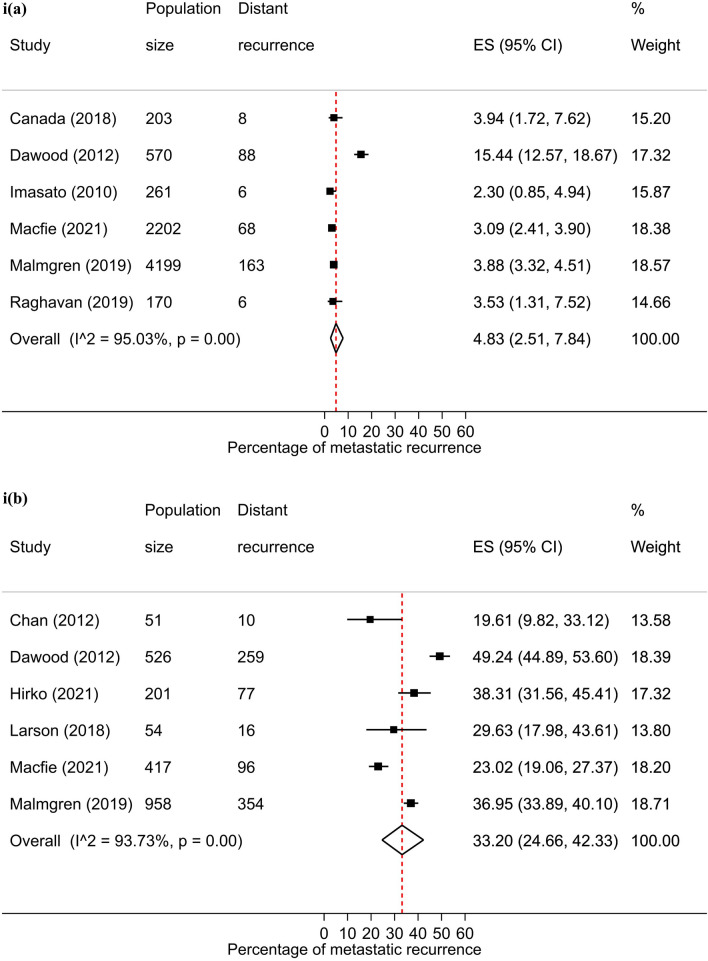
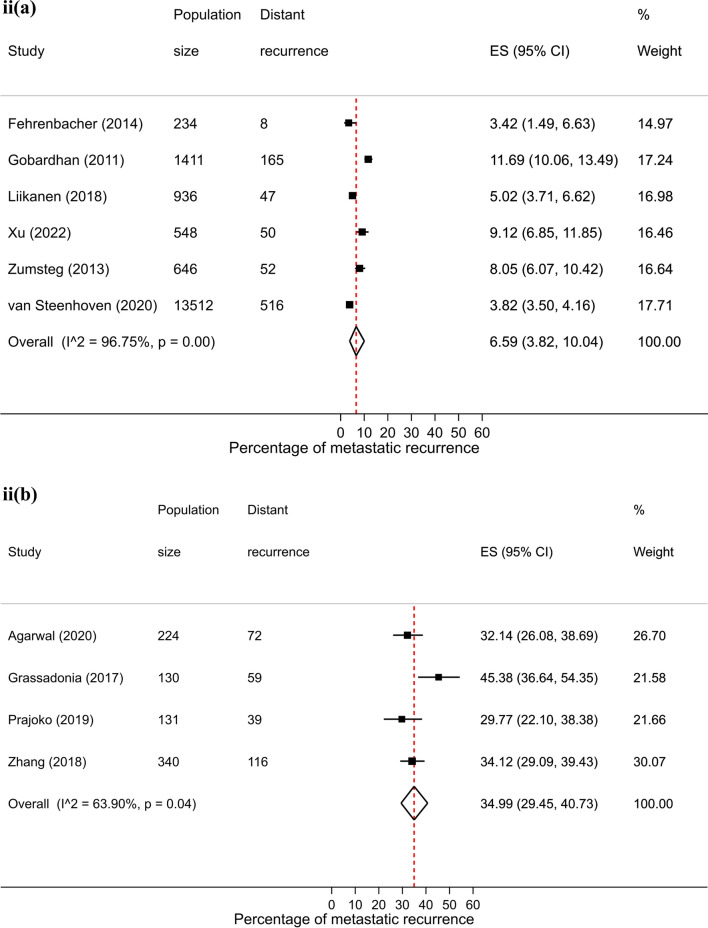
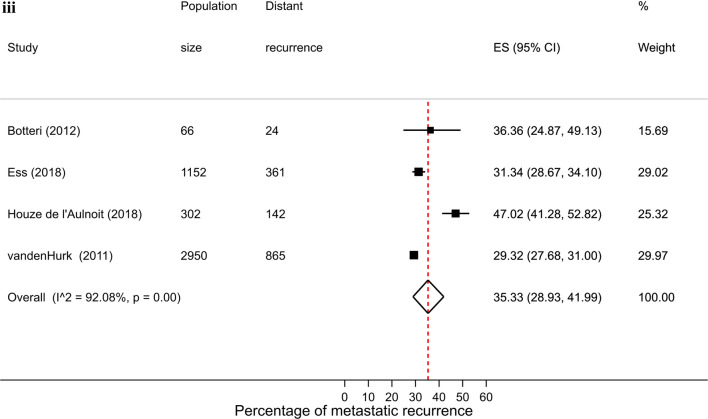
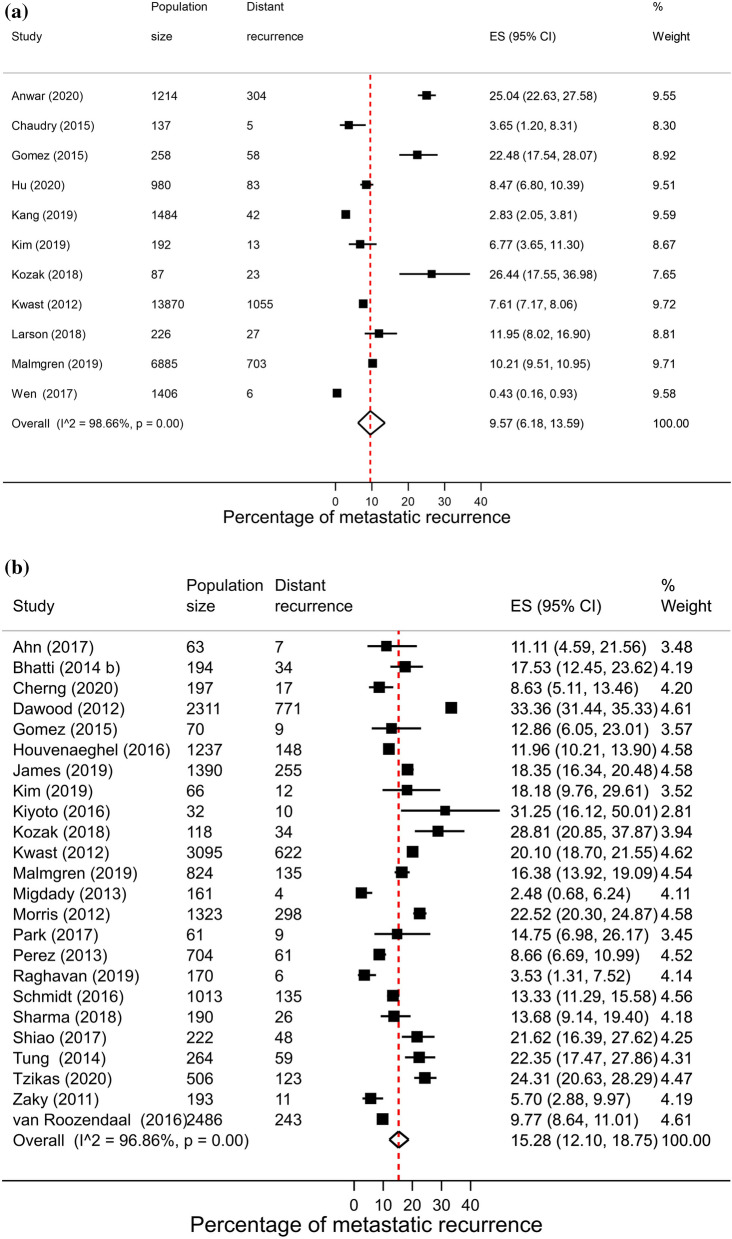
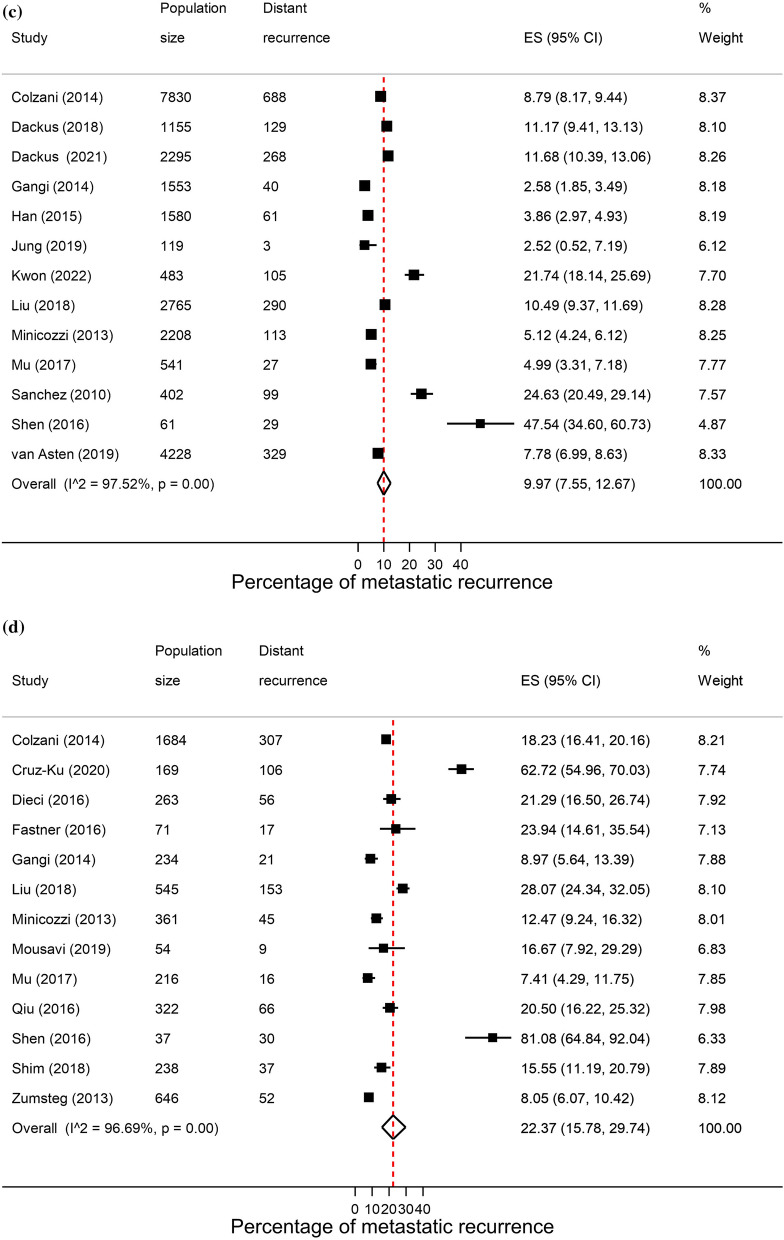
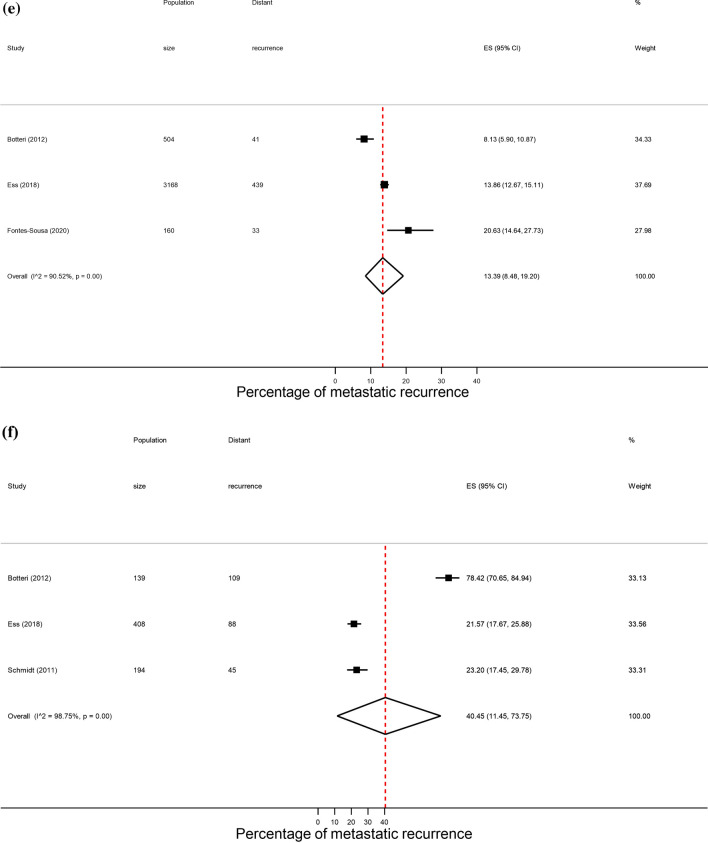
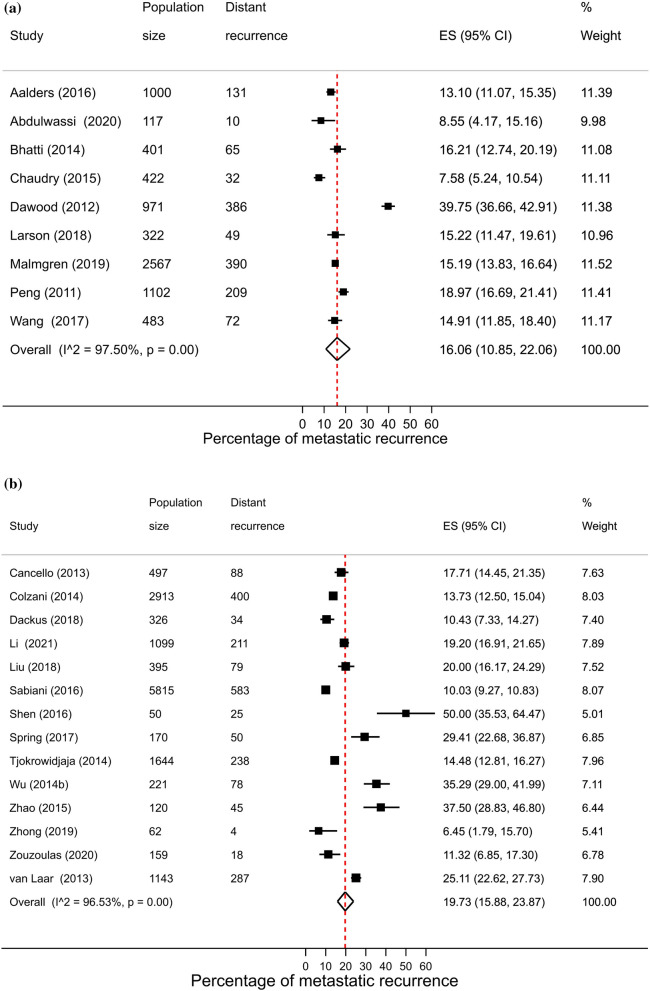
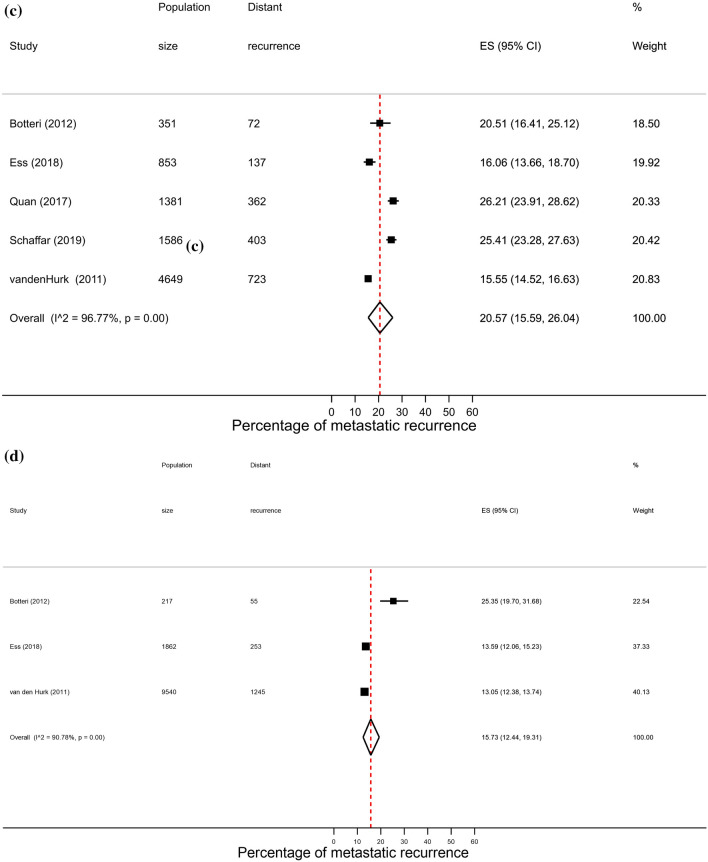
Results: 193 studies covering over 280,000 patients were included in the main analysis. Pooled proportions of metastatic recurrence increased with longer median follow-up time from 12.2% (95% CI 10.5-14.0%) at 1-4 years post diagnosis, 14.3% (95% CI 12.9-15.7%) at 5-9 years to 23.3% (95% CI 20.1-26.8) at 10 years or more. Regional variation was observed with pooled estimates ranging from 11.0% (95% CI 8.5-13.7%) in Europe to 26.4% (95% CI 16.7-37.4%) in Africa (1-4 years follow-up). Proportions of recurrence were higher in studies with diagnosis before 2000 (22.2%, 95% CI 15.1-30.3) compared to studies with diagnosis from 2000 onwards (12.8%, 95% CI 11.7-14.0). At 1-4 years median follow-up, pooled proportions of metastatic recurrence were higher in women with hormone receptor negative (15.2%, 95% CI 12.0-18.7%) compared with receptor positive disease (9.6%, 95% CI 6.2-13.6%) and in women with locally advanced (33.2%, 95% CI 24.7-42.3%) relative to early disease at initial diagnosis (4.8%, 95% CI 2.5-7.8%). Proportions were higher in those under 50 years compared with 70+ years, 18.6% (95% CI 15.9-21.4%) versus 13.3% (95% CI 9.2, 18.0%), respectively. Heterogeneity was high in all meta-analyses and results should be interpreted with caution.
Conclusions: Higher proportions of metastatic recurrence in patients initially diagnosed at an advanced stage and in earlier calendar period emphasises the importance of early detection and treatment advancements. As the global number of breast cancer survivors increases, research and health policy efforts should be directed towards timely diagnosis and access to effective treatments and care.
Study registration: PROSPERO CRD42022314500.
Keywords: Breast cancer; Meta-analysis; Metastasis; Recurrence; Systematic review.
© 2024. World Health Organization and the Authors 2024.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval was not required for this study because it used existing and aggregated non-identifiable data. Competing interests: Melina Arnold Employment: F. Hoffmann La Roche.
Figures
References
-
- Bray F, Laversanne M, Sung H, Ferlay J, Siegel R, Soerjomataram S, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians. 2024;74(3):229-63 - PubMed
-
- Global Cancer Observatory. https://gco.iarc.fr/. Accessed 27 Sep 2024.
-
- Coles CE, Earl H, Anderson BO, Barrios CH, Bienz M, Bliss JM, et al. The lancet breast cancer commission. The Lancet. 2024;403(10439):1895–950. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
