

Development and validation of a nomogram model for predicting the risk of hypertension in Bangladesh
- PMID: 39605842
- PMCID: PMC11600071
- DOI: 10.1016/j.heliyon.2024.e40246
Development and validation of a nomogram model for predicting the risk of hypertension in Bangladesh
Abstract
Background and objectives: Hypertension (HTN) is a leading cause of non-communicable disease in low- and middle-income countries, including Bangladesh. Thus, the objectives of this study were to investigate the associated risk factors for HTN and develop with validate a monogram model for predicting an individual's risk of HTN in Bangladesh.
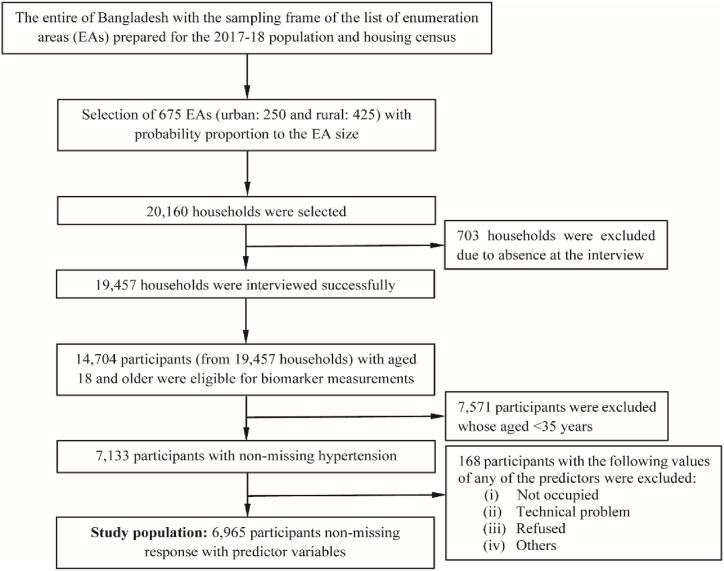
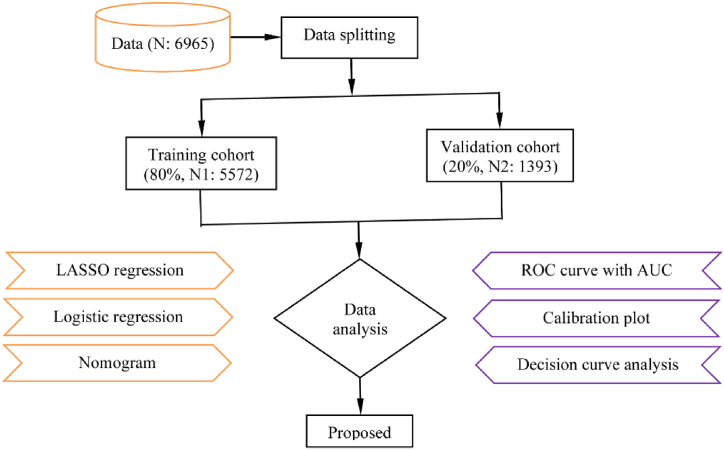
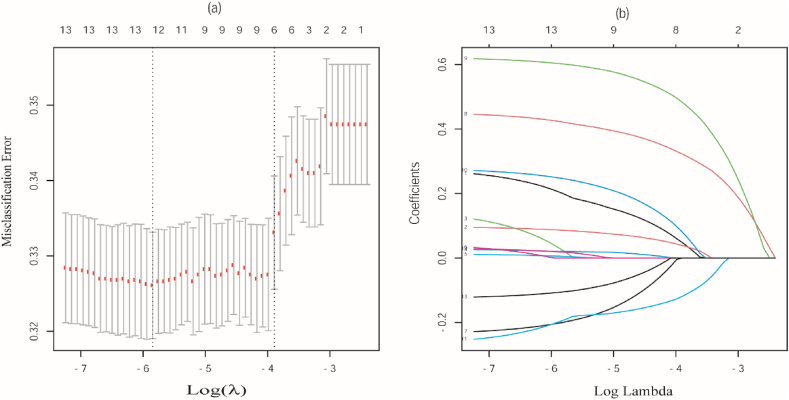
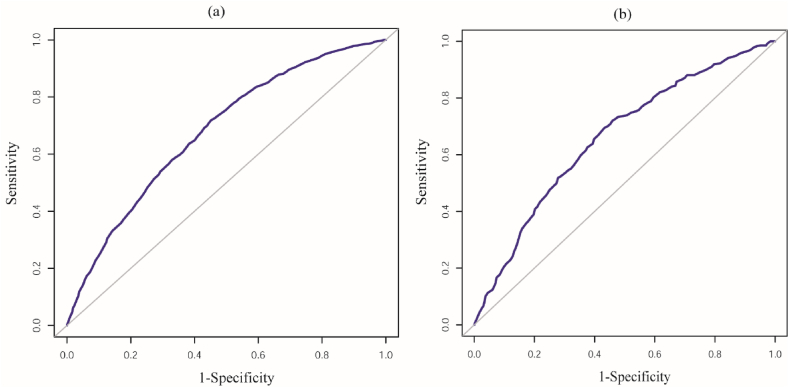
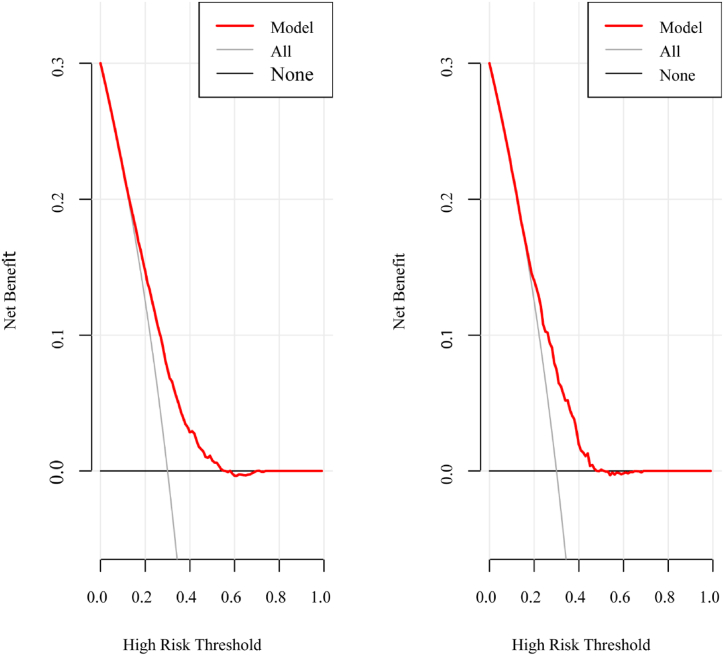
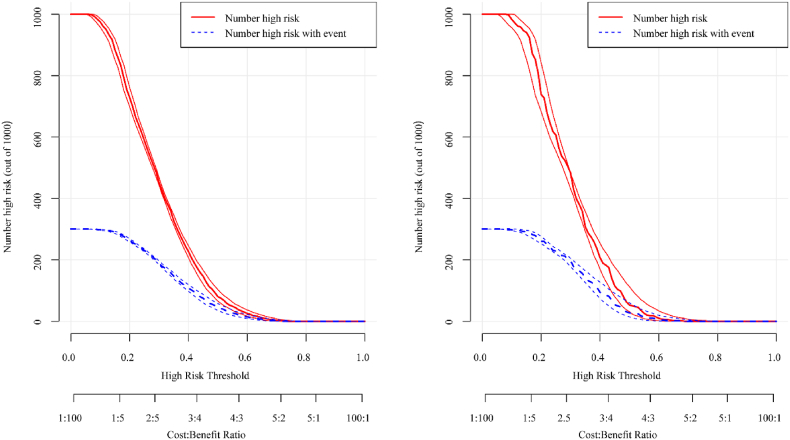
Materials and methods: This study exploited the latest nationally representative cross-sectional BDHS, 2017-18 data, which consisted of 6569 participants. LASSO and logistic regression (LR) analysis were performed to reduce dimensionality of data, identify the associated risk factors, and develop a nomogram model for predicting HTN risk in the training cohort. The discrimination ability, calibration, and clinical effectiveness of the developed model were evaluated using validation cohort in terms of area under the curve (AUC), calibration plot, decision curve analysis, and clinical impact curve analysis.
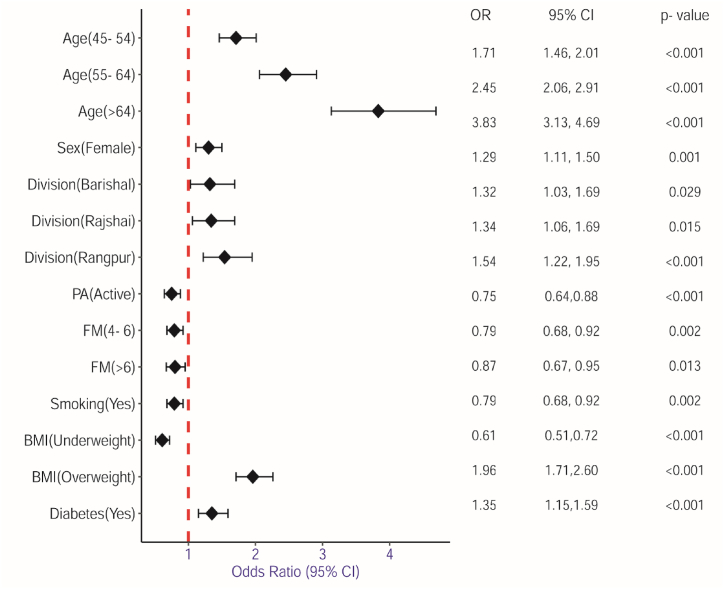
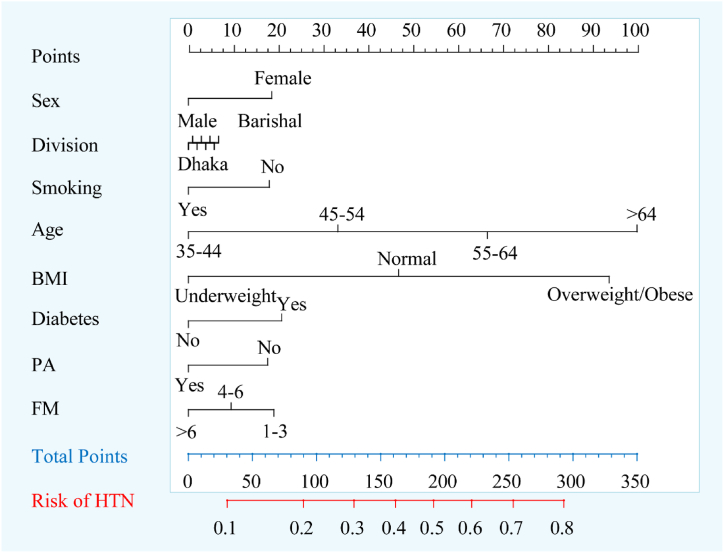
Results: The combined results of the LASSO and LR analysis demonstrated that age, sex, division, physical activity, family member, smoking, body mass index, and diabetes were the associated risk factors of HTN. The nomogram model achieved good discrimination ability with AUC of 0.729 (95 % CI: 0.685-0.741) for training and AUC of 0.715 (95 % CI: 0.681-0.729)] for validation cohort and showed strong calibration effects, with good agreement between the actual and predicted probabilities (p-value = 0.231).
Conclusion: The proposed nomogram provided a good predictive performance and can be effectively utilized in clinical settings to accurately diagnose hypertensive patients who are at risk of developing severe HTN at an early stage in Bangladesh.
Keywords: Bangladesh; Hypertension; LASSO; Logistic regression; Nomogram.
© 2024 The Authors. Published by Elsevier Ltd.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
LinkOut - more resources
Full Text Sources
