

This is a preprint.
Remoscope: a label-free imaging cytometer for malaria diagnostics
- PMID: 39606416
- PMCID: PMC11601755
- DOI: 10.1101/2024.11.12.24317184
Remoscope: a label-free imaging cytometer for malaria diagnostics
Update in
-
Remoscope: a label-free imaging cytometer for malaria diagnostics.Trans R Soc Trop Med Hyg. 2025 Sep 2;119(9):1100-1111. doi: 10.1093/trstmh/traf070. Trans R Soc Trop Med Hyg. 2025. PMID: 40631413
Abstract
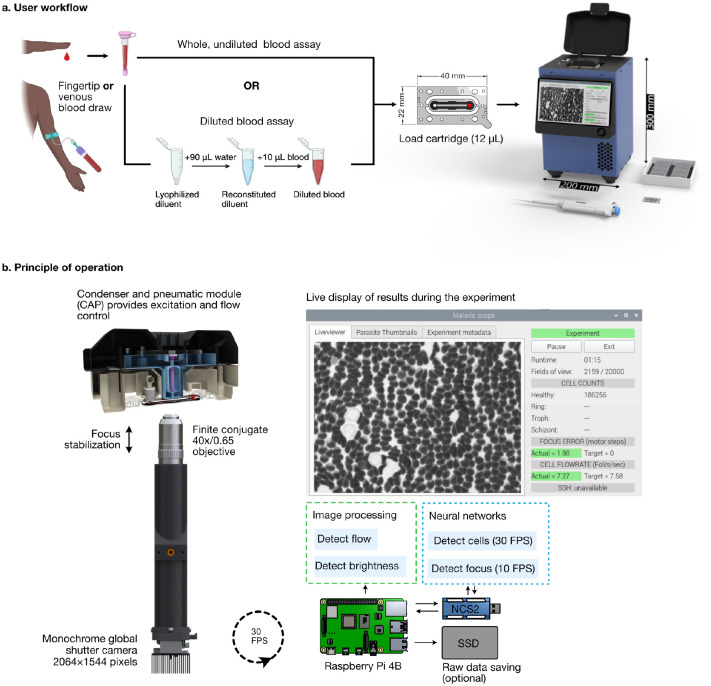
Malaria diagnostic testing in high transmission settings remains a burden on healthcare systems. Here we present Remoscope, a portable automated imaging cytometer that scans fresh, unstained whole blood using a custom neural network on low-cost hardware. By screening up to two million red blood cells, Remoscope performs label-free quantitative stage-specific detection of Plasmodium falciparum (Pf) in 1-12 minutes without sample fixation, staining, or slide scanning. Flow is used to achieve high cellular throughput, with blood confined to a 4.5 μm monolayer in low-cost disposable flow cartridges. Remoscope performance was benchmarked in vitro by titration of cultured parasites into uninfected whole blood at concentrations of 17.1-710,000 parasites/μL. Counts generated by Remoscope demonstrated a linear response across the entire range. Considering drug susceptibility assays, the half-maximal effective concentration (EC50) of chloroquine (CQ) for the W2 strain of Pf was 211 nM by Remoscope, compared to 191 nM for conventional flow cytometry. Remoscope's real-world diagnostic accuracy was evaluated in a cohort of 500 individuals in eastern Uganda, comprising 601 unique clinic visits. Parallel measurements of parasitemia were performed using Remoscope, qPCR targeting the multicopy conserved var gene acidic terminal sequence, and microscopic evaluation of Giemsa-stained thick blood smears. Remoscope's limit of detection with respect to qPCR was 95.1 parasites/μL. At this threshold, the system had a sensitivity of 83%, specificity of 96%, Positive Predictive Value (PPV) of 91%, and a Negative Predictive Value (NPV) of 93%. Remoscope's speed, accuracy, low cost, and ease of use address practical challenges in malaria diagnostic settings around the world. As a general imaging flow cytometer, Remoscope may also inform the development of recognition models for the diagnosis of other infectious and noninfectious blood disorders.
Keywords: Malaria; diagnostics; label-free imaging; machine learning.
Conflict of interest statement
Competing interests PML, RGS, and JLD declare international patent application No. PCT/US2021/047974.
Figures




References
-
- World malaria report 2023. Available at: https://www.who.int/teams/global-malaria-programme/reports/world-malaria... [Accessed 3 September 2024].
-
- World malaria report 2022. Available at: https://www.who.int/publications-detail-redirect/9789240064898 [Accessed 27 October 2023].
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials