

Enhancing multisensory rehabilitation of visual field defects with transcranial direct current stimulation: A randomized clinical trial
- PMID: 39607286
- PMCID: PMC11625917
- DOI: 10.1111/ene.16559
Enhancing multisensory rehabilitation of visual field defects with transcranial direct current stimulation: A randomized clinical trial
Abstract
Background and purpose: Visual rehabilitation is necessary for improving the quality of life of patients with acquired homonymous visual field defects (HVFDs). By modulating brain excitability and plasticity, transcranial direct current stimulation (tDCS) may accelerate and increase the effects of compensatory trainings, which are usually long and intensive. In the present proof-of-principle, double-blind, randomized, sham-controlled study, we assess whether anodal tDCS applied over ipsilesional occipital or parietal cortices can increase the effects of a compensatory audiovisual training for HVFDs.
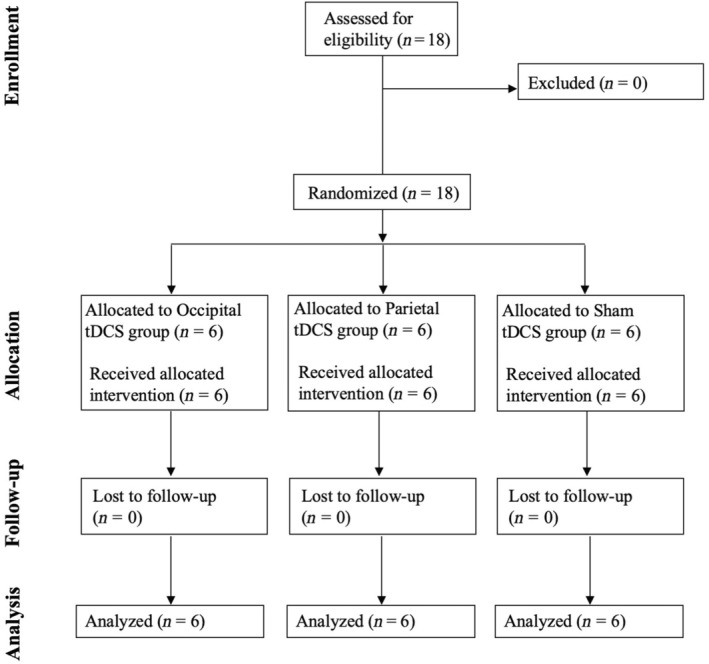
Methods: Eighteen participants with chronic HVFDs were randomized to receive anodal or sham tDCS over the ipsilesional parietal or occipital cortex during a 2-week (10 days, 2 h/day) audiovisual treatment aimed at improving oculomotor visual field exploration. Improvements were assessed by administering visual detection with eye movements and visual search tests, and a questionnaire for activities of daily living (ADLs) before the treatment, at its end, and at 1-month and 4-month follow-ups; lesion analyses were performed to look for predictors of treatment effects.
Results: Anodal ipsilesional tDCS, regardless of the target area (occipital vs. parietal), speeds up and increases daily improvements during the training. Whereas long-lasting (up to 4 months) post-treatment improvements in visual search and ADLs were observed in all groups, a greater and stable increase of visual detections in the blind hemifield was brought about only by the adjuvant use of occipital tDCS.
Conclusions: Compensatory audiovisual rehabilitation of HFVDs is effective and benefits from the adjuvant application of occipital and parietal tDCS, which speeds up and increases training-induced improvement.
Registry number: NCT06116760.
Keywords: hemianopia; rehabilitation; stroke; transcranial direct current stimulation.
© 2024 The Author(s). European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Zihl J. Rehabilitation of Visual Disorders after Brain Injury. 1st ed. Psychology Press; 2021. http://digital.casalini.it/9781000443271. doi: 10.4324/9781003210535 - DOI
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
