

Systematic review and meta-analysis comparing outcomes of multi-port versus single-incision laparoscopic surgery (SILS) in Hartmann's reversal
- PMID: 39607440
- PMCID: PMC11604776
- DOI: 10.1007/s00384-024-04752-2
Systematic review and meta-analysis comparing outcomes of multi-port versus single-incision laparoscopic surgery (SILS) in Hartmann's reversal
Abstract
Background: Colostomy formation as part of the Hartmann's procedure is often performed during emergency surgery as a damage limitation measure where attempts at bowel anastomosis and continuity are contraindicated. Hartmann's reversal (HR) remains challenging and can be attempted through open surgery and various minimally invasive techniques (laparoscopic and robotic platforms). We aimed to analyse outcomes of conventional multi-port laparoscopy (CL) versus single-incision approach (SILS) in patients undergoing HR.
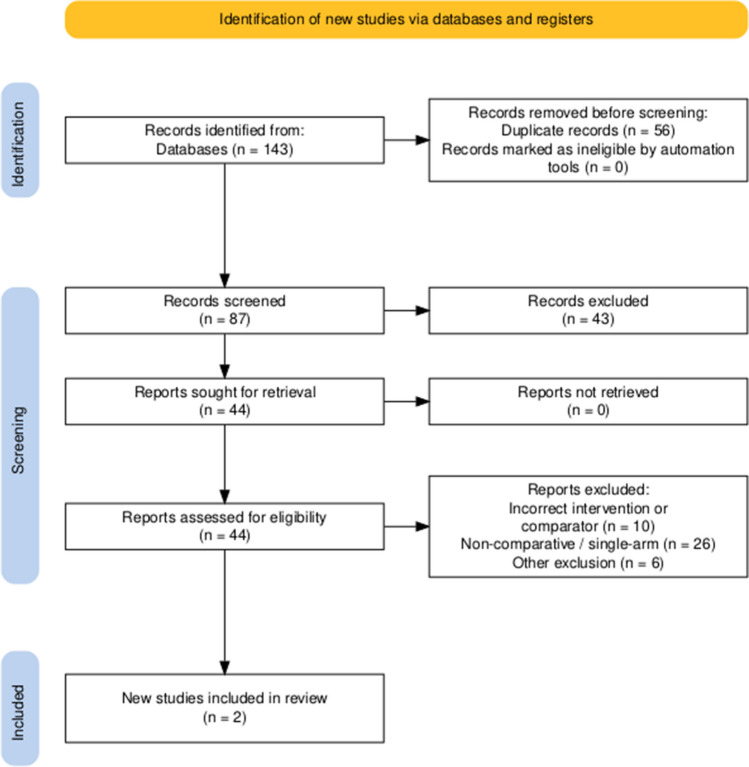
Methods: A comprehensive online search of various databases was conducted in accordance with PRISMA guidelines including Medline, PubMed, Embase, and Cochrane. Comparative studies of patients undergoing CL and SILS for HR were included. Analysed primary outcomes were total operative time and mortality rate. Secondary outcomes included post-operative complications, length of hospital stay, risk of visceral injury intra-operatively, and re-operation rate. Combined overall effect sizes were calculated using the random-effects model, and the Newcastle-Ottawa Scale (NOS) was used to assess bias.
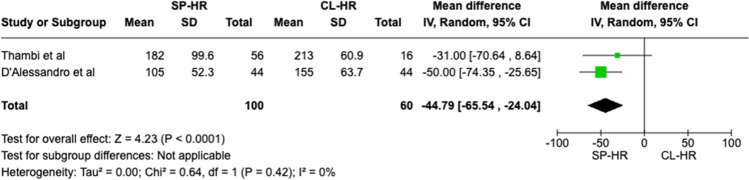
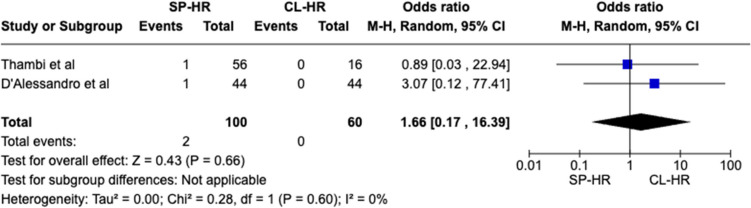
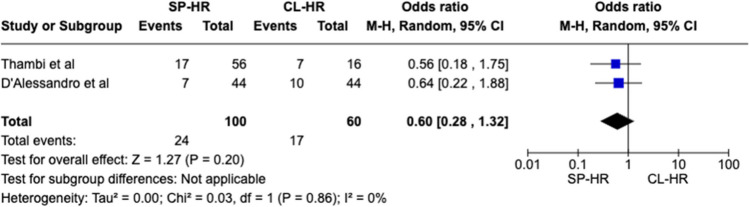
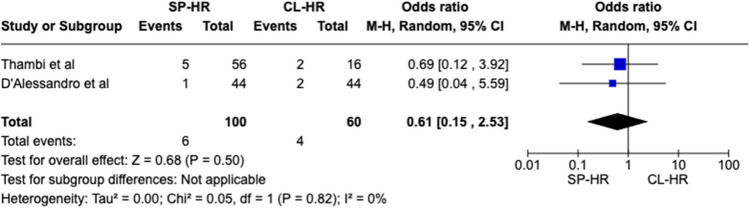
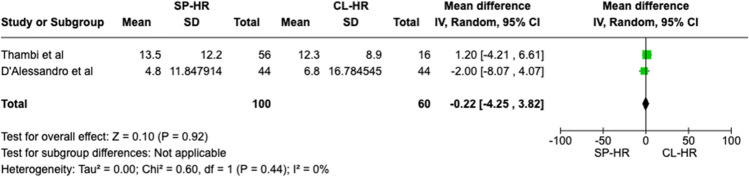
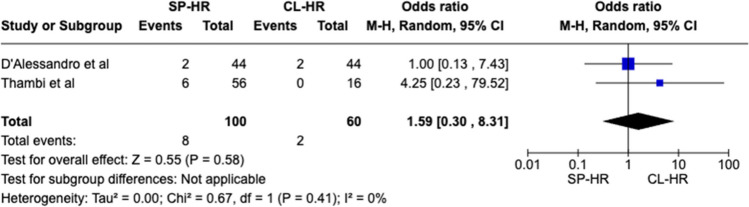
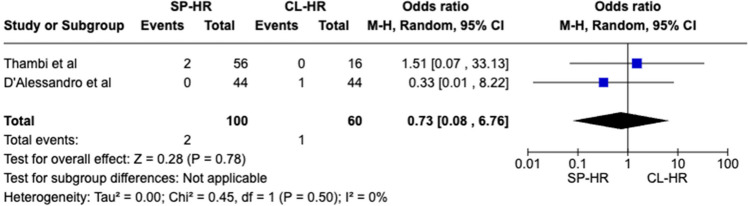
Results: Two observational studies matching our inclusion criteria with a total of 160 patients (SILS 100 vs. CL 60) were included. Statistical difference was observed for one outcome measure: operative duration (MD - 44.79 CI - 65.54- - 24.04, P < 0.0001). No significant difference was seen in mortality rate (OR 1.66 CI 0.17-16.39, P = 0.66), overall post-operative complications (OR 0.60 CI 0.28-1.32, P = 0.20), length of stay (MD - 0.22 CI - 4.25-3.82, P = 0.92), Clavien-Dindo III + complications (OR 0.61 CI 0.15-2.53, P = 0.50), risk of visceral injury (OR 1.59 CI 0.30-8.31, P = 0.58), and re-operation rates (OR 0.73 CI 0.08-6.76, P = 0.78).
Conclusion: Accounting for study limitations, the SILS procedure seems to be quicker with non-inferior outcomes compared with the conventional multi-port approach. This may lead to better patient satisfaction and cosmesis and potentially reduce the risk of future incisional hernia occurrence. However, well-designed, randomised studies are needed to draw more robust conclusions and recommendations.
Keywords: Colostomy reversal; Laparoscopy; Multi-port; SILS.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: This study was a meta-analysis of published data so no prior ethical approval was required. Conflict of interest: The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
