

Griscelli Syndrome Type 2: Comprehensive Analysis of 149 New and Previously Described Patients with RAB27A Deficiency
- PMID: 39607447
- PMCID: PMC11604824
- DOI: 10.1007/s10875-024-01842-2
Griscelli Syndrome Type 2: Comprehensive Analysis of 149 New and Previously Described Patients with RAB27A Deficiency
Abstract
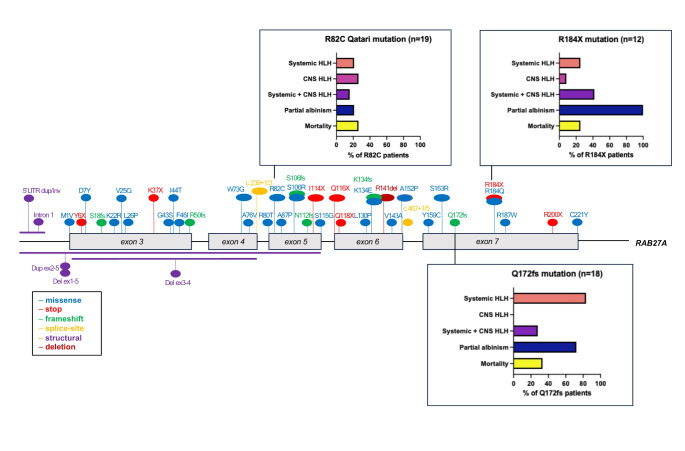
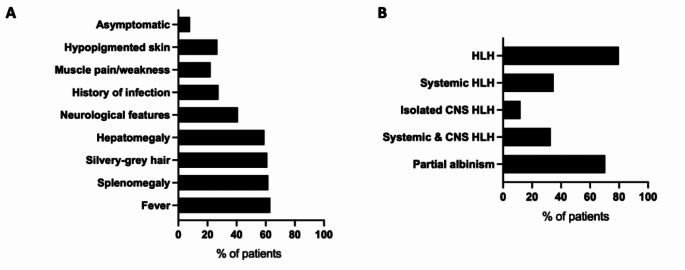
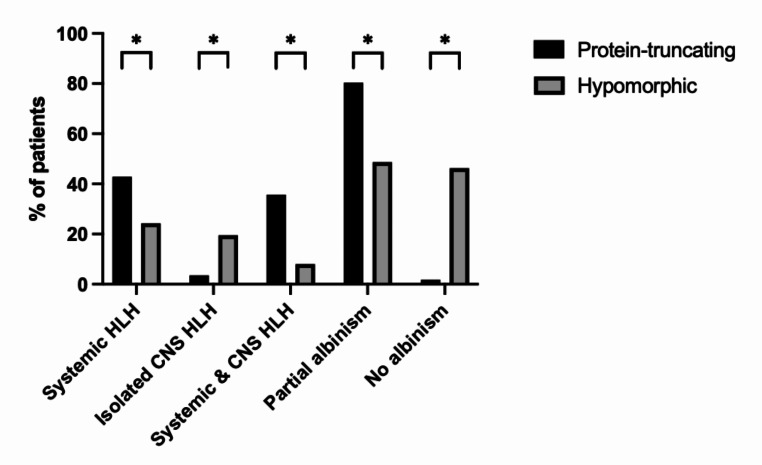
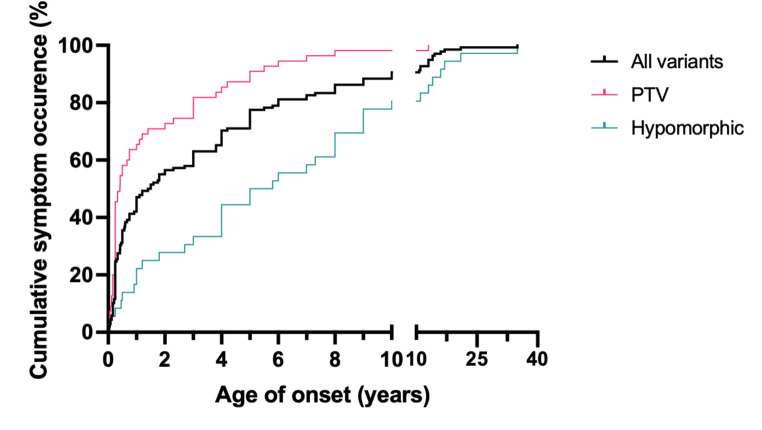
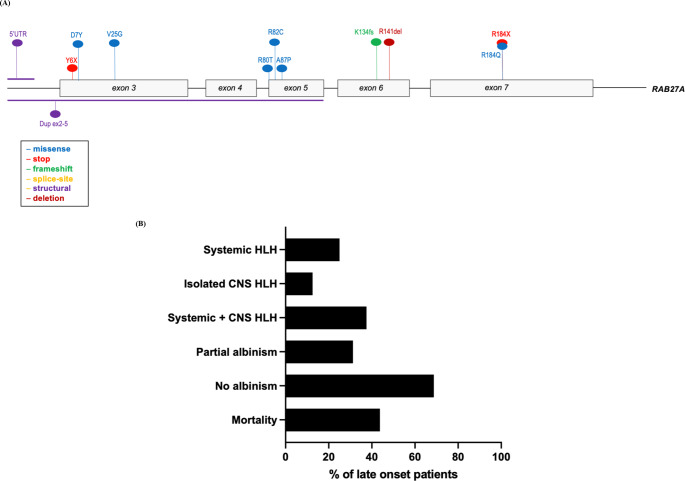
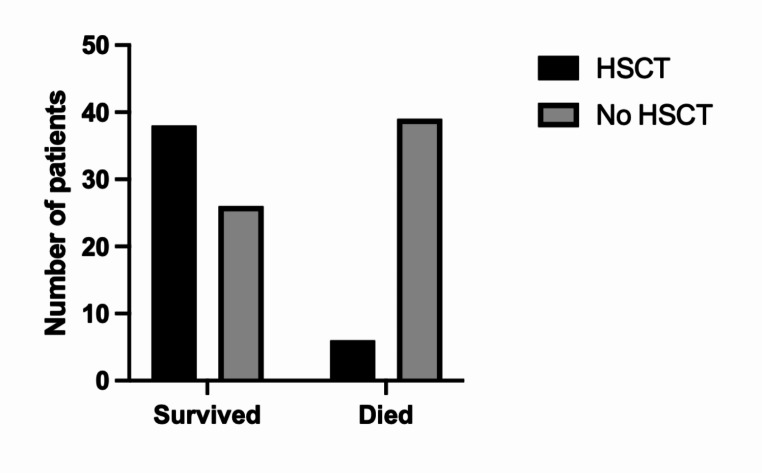
Griscelli syndrome type 2 (GS2) is a rare, life-threatening immunodysregulatory disorder characterised by impaired cytotoxic activity leading to susceptibility to haemophagocytic lymphohistiocytosis (HLH) and hypopigmentation. We completed a literature review and analysis of clinical data of 149 patients with GS2 including 8 new patients.We identified three founder mutations which show diverse phenotypic profiles (RAB27A c.244 C > T, p.R82C, c.514_518delCAAGC, p.Q172NfsX2, c.550 C > T, p.R184X). The most common presentation was HLH (119/149, 80%), with high proportion of central nervous system involvement (68/149, 46%). Features of partial albinism were present in 105 of 149 cases (70%). Hypopigmentation can be absent in GS2 and should not exclude the diagnosis. Patients with biallelic protein truncating variants (PTV) were more likely to have systemic HLH (44/56, 79%) and partial albinism (45/56, 80%), in comparison to hypomorphic variants (9/41, 22%; 20/41, 49%). Patients with hypomorphic variants presented later (5.4 years cf. 0.4 years, p = < 0.0001) and were more likely to have isolated CNS HLH (2% cf. 42%, p = 0.001).Mortality was high in the cohort (50/149, 34%). Survival of cases post-HLH who underwent transplantation is superior to un-transplanted patients, suggesting adequate HLH control followed by early HSCT is highly beneficial. Mortality was reduced in HSCT recipients versus the un-transplanted group where follow-up data was available (14% compared to 58%).Asymptomatic cases identified through family history/genetic screening may benefit from pre-emptive HSCT, but access and development of robust functional testing are required. High mortality related to HLH remains concerning and emphasises the need for improved molecular characterisation and clinical prognostic factors to guide management decisions.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing Interests: Dr Lim reported receiving personal fees from Octapharma, Roche, Novartis, and Amgen. All other authors have no conflict of interest to disclose.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
