

Traditional risk factors, optimal cardiovascular health, and elevated lipoprotein(a)
- PMID: 39607751
- PMCID: PMC12172025
- DOI: 10.1093/eurjpc/zwae382
Traditional risk factors, optimal cardiovascular health, and elevated lipoprotein(a)
Abstract
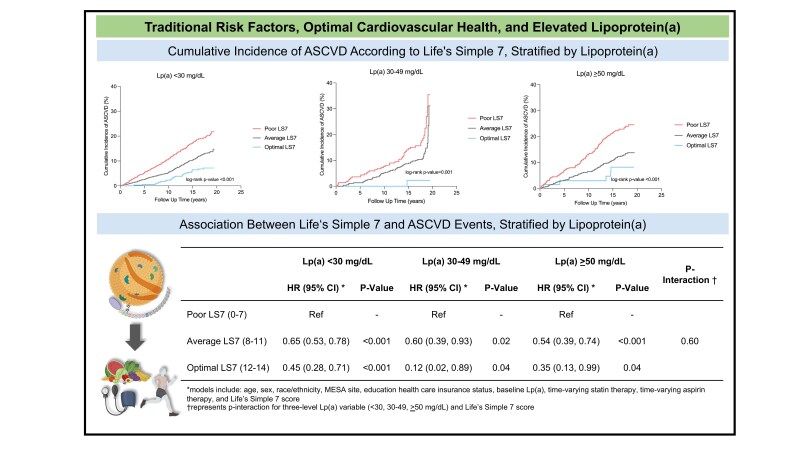
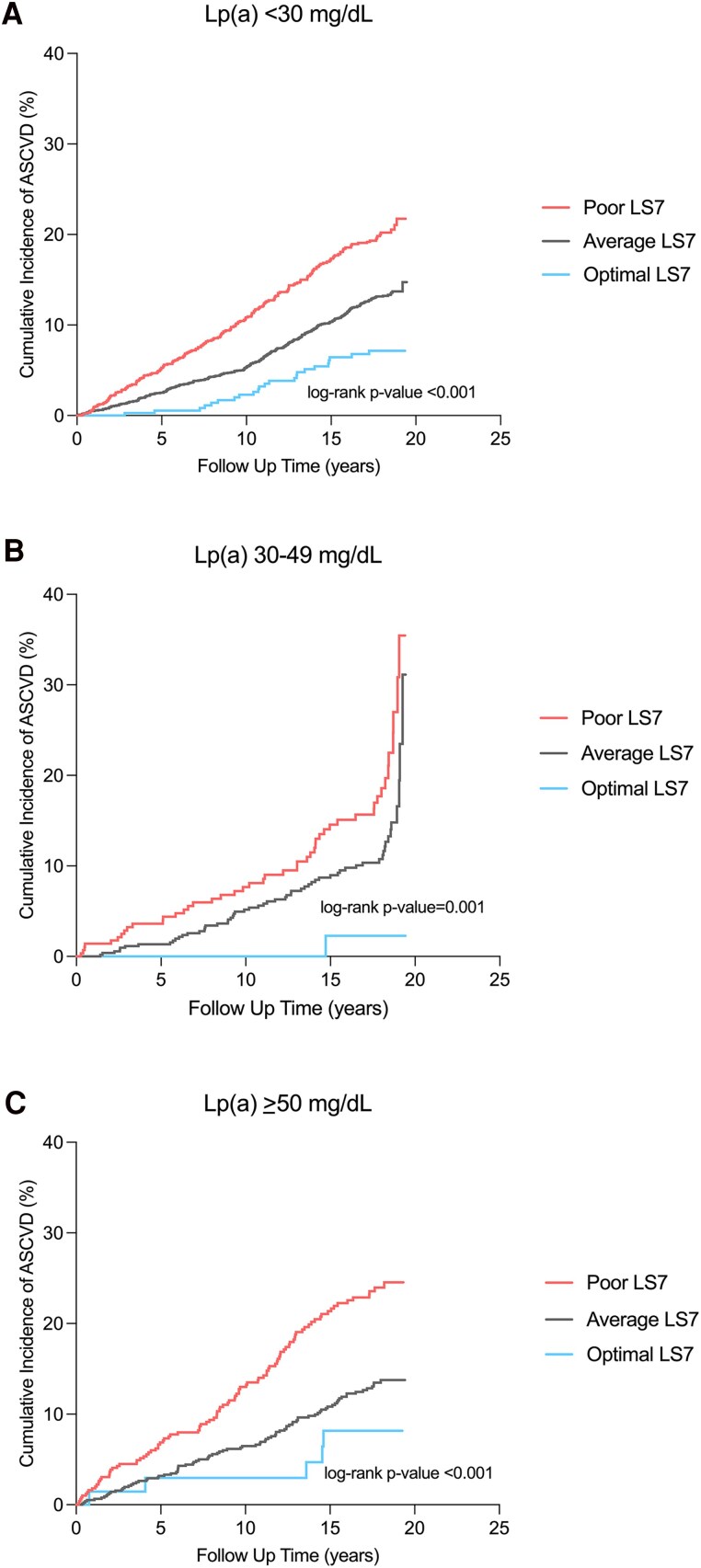
Aims: To assess the association of traditional risk factor burden and Life's Simple 7 (LS7) score with incident atherosclerotic cardiovascular disease (ASCVD) across lipoprotein(a) [Lp(a)] levels.
Methods and results: There were 6676 participants without clinical ASCVD from the Multi-Ethnic Study of Atherosclerosis who underwent Lp(a) testing and were followed for incident ASCVD events (coronary heart disease and stroke). Low, intermediate, and elevated Lp(a) were defined as <30, 30-49, and ≥50 mg/dL, respectively. Cox proportional hazards regression assessed the association of traditional risk factors and LS7 score (poor: 0-8, average: 9-10, and optimal: 11-14) with incident ASCVD across Lp(a) groups during a median follow-up of 17.7 years, adjusting for demographics and time-varying statin and aspirin therapy. The mean age was 62.1 years, 53% were women, and 61% were non-white. The median Lp(a) was 17 (interquartile range 8-41) mg/dL, 13% had Lp(a) 30-49 mg/dL, and 20% had Lp(a) ≥ 50 mg/dL. Individuals with Lp(a) ≥ 50 mg/dL had higher absolute event rates across all LS7 categories. There was no significant interaction between Lp(a) and LS7 score on incident ASCVD (P-interaction = 0.60). Compared to a poor LS7 score, optimal LS7 conferred a lower risk for incident ASCVD among individuals with Lp(a) < 30 [hazard ratio (HR) = 0.45, 95% confidence interval (CI): 0.28-0.71], Lp(a) 30-49 (HR = 0.12, 95% CI: 0.02-0.89), and Lp(a) ≥ 50 mg/dL (HR = 0.35, 95% CI: 0.13-0.99).
Conclusion: Participants without clinical ASCVD who achieved an optimal LS7 score had ASCVD risk reduction regardless of Lp(a) level. These results emphasize the importance of a healthy lifestyle and ASCVD risk factor control among individuals with elevated Lp(a).
Keywords: American Heart Association; Cardiovascular disease; Cholesterol; Lifestyle; Lipoprotein(a); Prevention.
Plain language summary
Participants without clinical atherosclerotic cardiovascular disease (ASCVD) who achieved an optimal Life’s Simple 7 (LS7) score had ASCVD risk reduction regardless of lipoprotein(a) [Lp(a)] level.Compared to a poor LS7 score, an optimal LS7 score conferred a 55–88% lower ASCVD risk regardless of Lp(a) level.These results emphasize the importance of a healthy lifestyle and optimal ASCVD risk factor control among patients with elevated Lp(a).
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com.
Conflict of interest statement
Conflict of interest: H.S.B. is a consultant/advisor for Kaneka, Novartis, Arrowhead, and Abbott. S.T. is a co-inventor and receives royalties from patents owned by UCSD, is a co-founder and has an equity interest in Oxitope and Kleanthi Diagnostics, and is a consult to Novartis and has a dual appointment at UCSD and Ionis Pharmaceuticals. The terms of this arrangement have been reviewed and approved by the University of California, San Diego in accordance with its conflict-of-interest policies. The other co-authors have nothing to disclose.
Figures

References
-
- Reyes-Soffer G, Ginsberg HN, Berglund L, Duell PB, Heffron SP, Kamstrup PR, et al. Lipoprotein(a): a genetically determined, causal, and prevalent risk factor for atherosclerotic cardiovascular disease: a scientific statement from the American Heart Association. Arterioscler Thromb Vasc Biol 2022;42:e48–e60. - PMC - PubMed
-
- Malick WA, Goonewardena SN, Koenig W, Rosenson RS. Clinical trial design for lipoprotein(a)-lowering therapies: JACC Focus Seminar 2/3. J Am Coll Cardiol 2023;81:1633–1645. - PubMed
-
- Sc S, Sperling L, Virani SS, Yeboah J. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2019;73:e285–e350. - PubMed
-
- Lloyd-Jones DM, Morris PB, Ballantyne CM, Birtcher KK, Covington AM, DePalma SM, et al. 2022 ACC expert consensus decision pathway on the role of nonstatin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk: a report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol 2022;80:1366–1418. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- NCATS
- 75N92020D00001/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- 75N92020D00001/NH/NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- L30 HL175751/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- K08 HL166962/HL/NHLBI NIH HHS/United States
- 75N92020D00005/NH/NIH HHS/United States
- 75N92020D00002/HL/NHLBI NIH HHS/United States
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/NH/NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- 75N92020D00005/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- UL1-TR-000040, UL1-TR-001079/HL/NHLBI NIH HHS/United States
- L30HL175751/NH/NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01-HC-95160, 75N92020D00002, N01-HC-95161, 75N92020D00003, N01-HC-95162, 75N92020D00006, N01-HC-95163, 75N92020D00004, N01-HC-95164, 75N92020D00007, N01-HC-95165, N01-HC-95166, N01-HC-95167, N01-HC-95168/NH/NIH HHS/United States
- NIH
- N01-HC-95169/NH/NIH HHS/United States
- R01 HL170224/HL/NHLBI NIH HHS/United States
- 1K08HL166962/NH/NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- 75N92020D00003/HL/NHLBI NIH HHS/United States
- N01-HC-95159/NH/NIH HHS/United States
- U.S. Department of Health and Human Services
- UL1-TR-001420/HL/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- 75N92020D00004/HL/NHLBI NIH HHS/United States
- F32 HL172499/HL/NHLBI NIH HHS/United States
- R01 HL159156/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- 75N92020D00007/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- F32HL172499/NH/NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- 75N92020D00006/HL/NHLBI NIH HHS/United States
- HL170224/HB/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
