

New diagnostic approach to central hypothyroidism after traumatic brain injury in children and adolescents
- PMID: 39608103
- PMCID: PMC11816043
- DOI: 10.1530/ETJ-24-0184
New diagnostic approach to central hypothyroidism after traumatic brain injury in children and adolescents
Abstract
Background: Pituitary lesions after traumatic brain injury (TBI) are frequent in children and adolescents, but the rate of post-TBI central hypothyroidism remains uncertain.
Objective: To identify the long-term incidence of post-TBI CH and the clinical and laboratory characteristics of this complication in children and adolescents.
Methods: The analysis included 31 patients with a history of TBI with at least 1 year of follow-up. Patients were evaluated at hospital admission and every 3 months thereafter. Assessments included clinical evaluation, brain CT and hormone assessments (basal fT4, IGF-1, cortisol and adrenocorticotropic hormone; insulin tolerance test/thyrotropin-releasing hormone test with TSH, growth hormone and cortisol measurement; and corticotropin-releasing hormone test, if indicated). The CH diagnosis was based on clinical and laboratory findings and a therapeutic trial with levothyroxine.
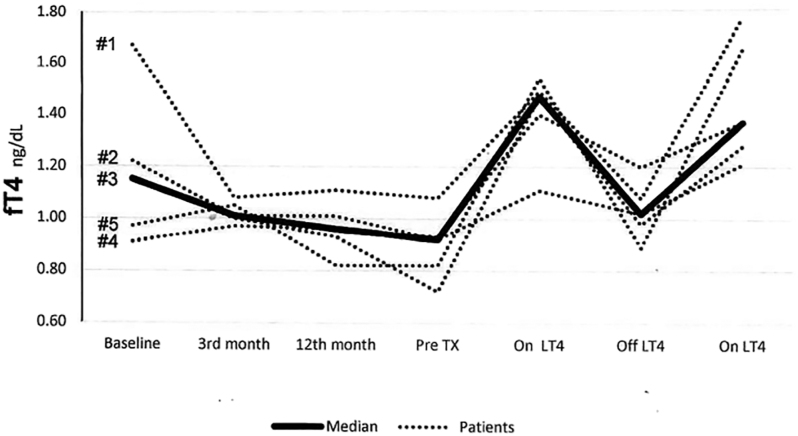
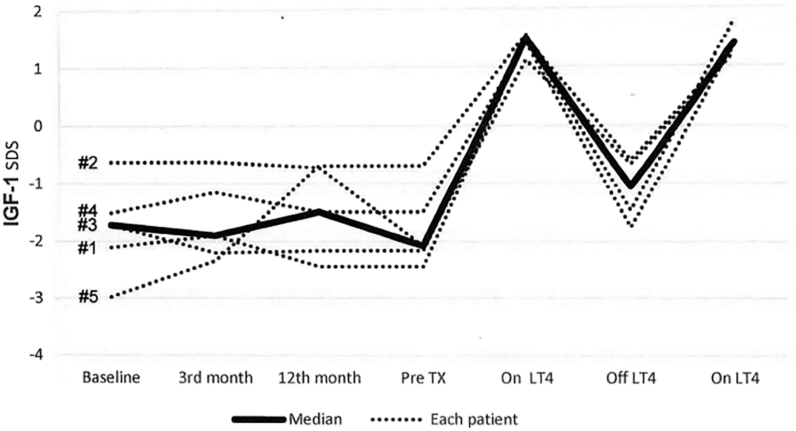
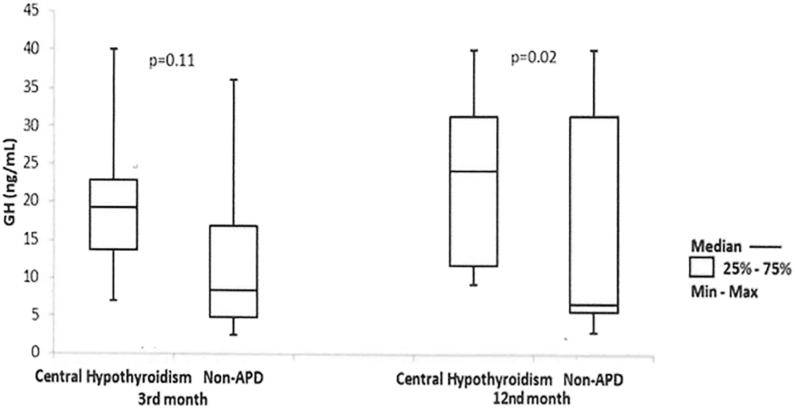
Results: Overall, five patients (16%) developed CH (3 with associated adrenal insufficiency). At 3 and 12 months, median fT4 values were lower in patients with CH compared with those without anterior pituitary dysfunction (n = 18; P = 0.01). Patients with CH received levothyroxine and progressed with clinical resolution and increased median fT4 (from 0.92 to 1.47 ng/dL) and IGF-1 (from -2.08 to -0.22 standard deviation scores (SDS)) levels. Temporary suspension of levothyroxine was accompanied by decreased median fT4 (1.02 ng/dL) and IGF-1 (-1.07 SDS) levels and reappearance of clinical symptoms, which resolved once levothyroxine was reinitiated.
Conclusions: The longer follow-up, valorization of clinical manifestations, nontraditional laboratory approach and therapeutic trial with levothyroxine in the present study revealed a higher rate of post-TBI CH in children and adolescents than that reported in the literature.
Keywords: GH; IGF-1; adolescents; central hypothyroidism; children; traumatic brain injury.
Conflict of interest statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the work.
Figures
References
-
- Ceballos R. Pituitary changes in head trauma (analysis of 102 consecutive cases of head injury). Ala J Med Sci 1966. 3 185–198. - PubMed
-
- Cyran E. Hypophysenschädigung durch schädelbasisfraktur. Dtsch Med Wschr 1918. 44 1261.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
