

High level of circulating cell-free tumor DNA at diagnosis correlates with disease spreading and defines multiple myeloma patients with poor prognosis
- PMID: 39609411
- PMCID: PMC11605000
- DOI: 10.1038/s41408-024-01185-6
High level of circulating cell-free tumor DNA at diagnosis correlates with disease spreading and defines multiple myeloma patients with poor prognosis
Abstract
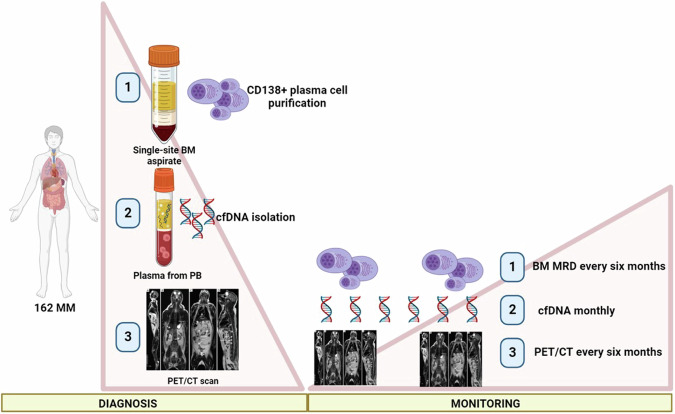
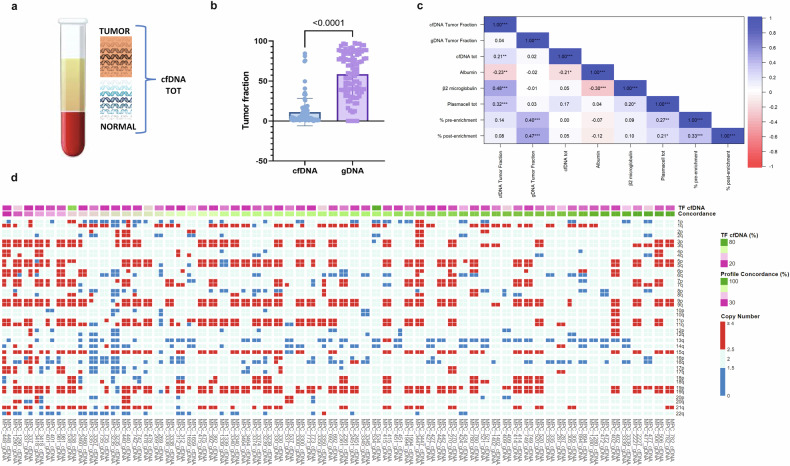
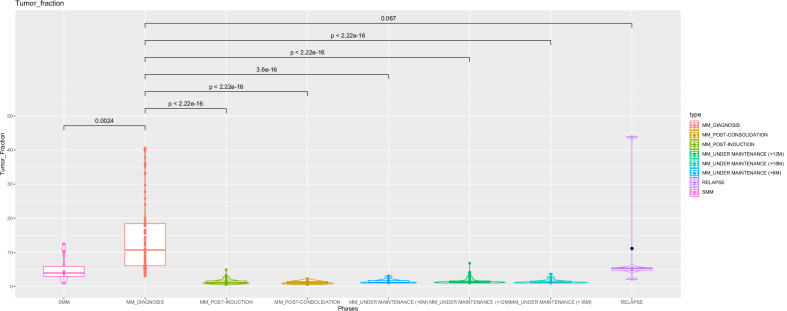
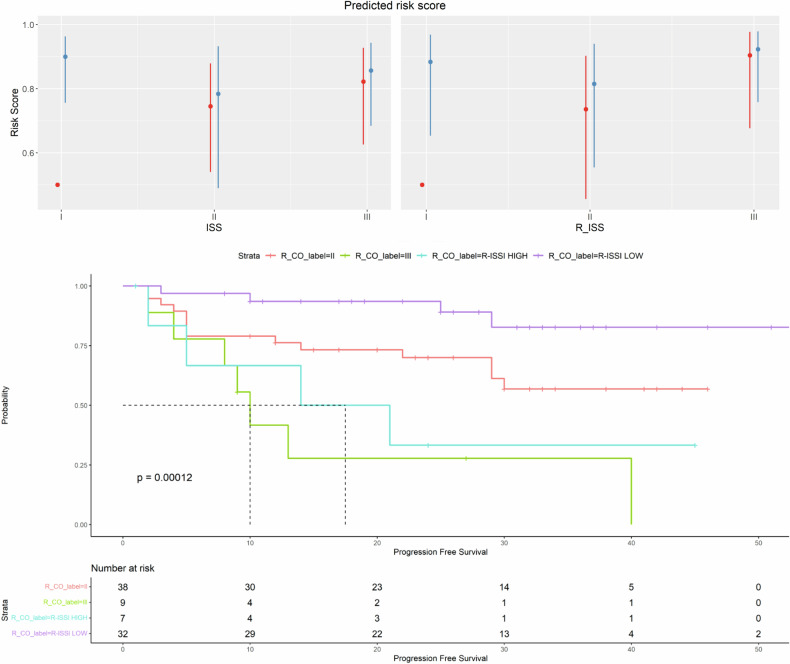
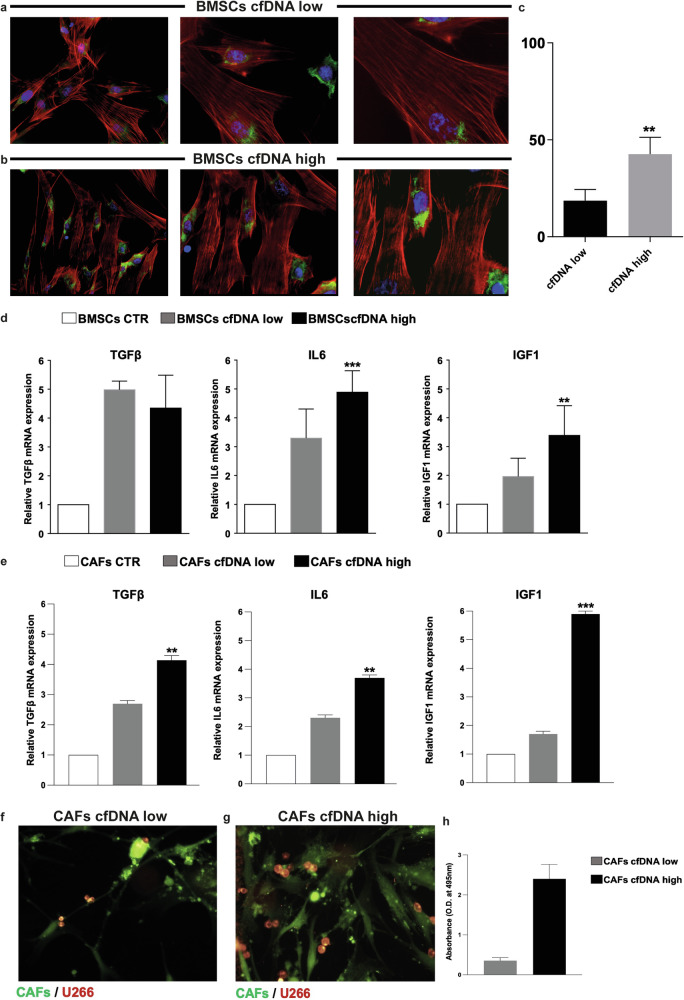
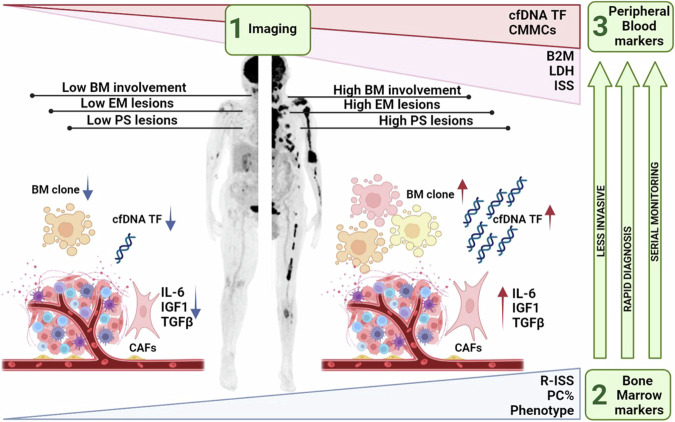
Multiple myeloma (MM) is a plasma cell (PC) disorder characterized by skeletal involvement at the time of diagnosis. Recently, cell-free DNA (cfDNA) has been proven to recapitulate the heterogeneity of bone marrow (BM) disease. Our aim was to evaluate the prognostic role of cfDNA at diagnosis according to disease distribution, and to investigate the role of the MM microenvironment inflammatory state in supplying the release of cfDNA. A total of 162 newly diagnosed MM patients were screened using 18F-FDG PET/CT and assessed by ultra low-pass whole genome sequencing (ULP-WGS). High cfDNA tumor fraction (ctDNA) levels were correlated with different tumor mass markers, and patients with high ctDNA levels at diagnosis were more likely to present with metabolically active paraskeletal (PS) and extramedullary (EM) lesions. Moreover, we demonstrated that microenvironment cancer-associated fibroblast (CAFs)-mediated inflammation might correlate with high ctDNA levels. Indeed, a high cfDNA TF level at diagnosis predicted a poorer prognosis, independent of R-ISS III and 1q amplification; the inclusion of >12% ctDNA in the current R-ISS risk score enables a better identification of high-risk patients. ctDNA can be a reliable and less invasive marker for disease characterization, and can refine patient risk.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests. Informed consent: All patients provided written informed consent for biological studies (Ethical Committee n. 167/2019/Sper/AUOBo).
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
