

The outcome of thrombotic microangiopathy in kidney transplant recipients
- PMID: 39609684
- PMCID: PMC11606107
- DOI: 10.1186/s12882-024-03846-x
The outcome of thrombotic microangiopathy in kidney transplant recipients
Abstract
Background: The outcome of kidney transplant recipients with a history of complement-mediated thrombotic microangiopathy (cTMA) and those who develop post-transplant de novo TMA (dnTMA) is largely unknown.
Methods: We retrospectively studied all kidney transplant recipients with end-stage kidney disease secondary to cTMA and those who developed dnTMA, between Jan 2000 and Dec 2020 in our center.
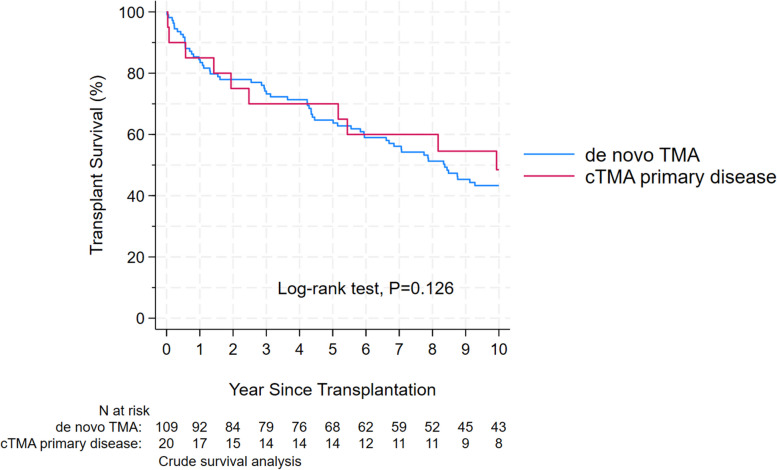
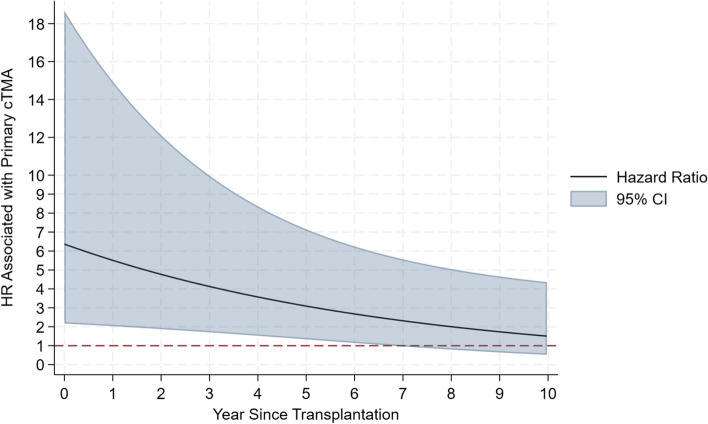
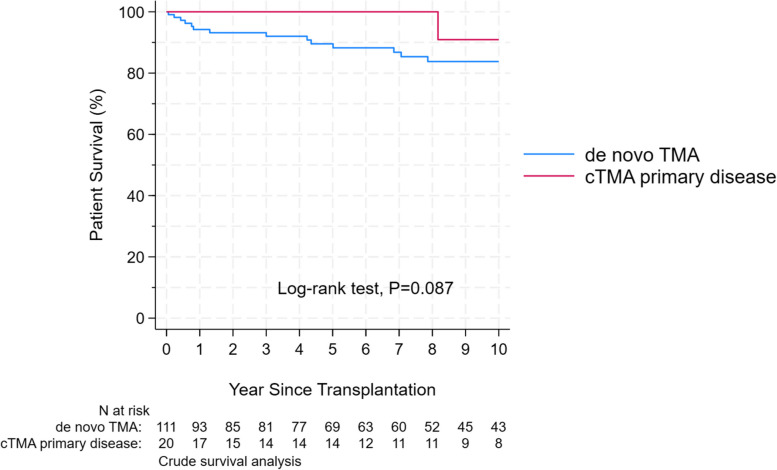
Results: We identified 134 patients, 22 with cTMA and 112 had dnTMA. Patients with cTMA were younger at the time of TMA diagnosis (age at diagnosis, 28.9 ± 16.3. vs 46.5 ± 16.0 years; P < 0.001). T-cell mediated rejection, borderline rejection, and calcineurin inhibitor toxicity were more prevalent in the first kidney transplant biopsy (P < 0.05) in the dnTMA group, and antibody-mediated rejection was more prevalent in anytime-biopsy (P = 0.027). After adjusting for potential confounders, cTMA was associated with a sixfold increase in the hazard of transplant failure during the first-year post-transplant (adjusted hazard ratio (aHR): 6.37 [95%CI: 2.17 to18.68; P = 0.001]; the aHR decreased by 0.87 (95% CI: 0.76 to 0.99: P = 0.033) per year elapsed since transplantation. Long-term allograft survival was similar in both groups.
Conclusion: Post kidney transplant TMA is an important cause of poor allograft survival. More studies are needed to enhance our understanding and management of this disorder.
Keywords: Complement-mediated TMA; De novo TMA; Kidney; Thrombotic Microangiopathy; Transplant.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The ethics committee is the Johns Hopkins Hospital’s Institutional Review Board. This is a retrospective study, data were collected from the electronic medical records, consents were waived by Johns Hopkins Hospital’s Institutional Review Board. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Hariharan S, Israni AK, Danovitch G. Long-Term Survival after Kidney Transplantation. N Engl J Med. 2021Aug 19;385(8):729–43. - PubMed
-
- Moake JL. Thrombotic microangiopathies. N Engl J Med. 2002Aug 22;347(8):589–600. - PubMed
-
- Zarifian A, Meleg-Smith S, O’donovan R, Tesi RJ, Batuman V. Cyclosporine-associated thrombotic microangiopathy in renal allografts. Kidney Int. 1999 Jun;55(6):2457–66. - PubMed
-
- Reynolds JC, Agodoa LY, Yuan CM, Abbott KC. Thrombotic microangiopathy after renal transplantation in the United States. Am J Kidney Dis. 2003Nov;42(5):1058–68. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
