

Neoadjuvant therapy in rectal cancer-one year follow-up results of standard versus total neoadjuvant strategies
- PMID: 39609915
- PMCID: PMC11603888
- DOI: 10.1186/s12957-024-03590-4
Neoadjuvant therapy in rectal cancer-one year follow-up results of standard versus total neoadjuvant strategies
Abstract
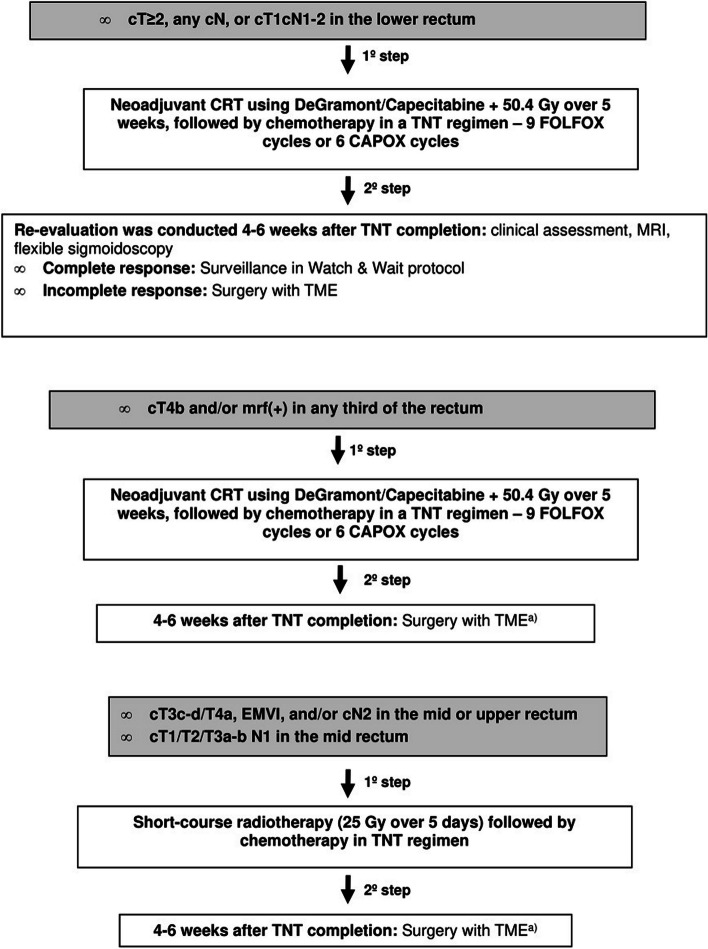
Background: Locally advanced rectal cancer (LARC) poses a significantly challenge in clinical management, requiring a multimodal treatment approach. Among innovative strategies, Total Neoadjuvant Therapy (TNT) has emerged, delivering all planned chemotherapy before surgery.
Objective: Our aim was to evaluate the real-world application and efficacy of TNT and to compare it with the non-TNT standard strategy.
Methods: This retrospective study compared locally advanced rectal adenocarcinoma patients treated with Total Neoadjuvant Therapy (TNT) in 2022 with those who underwent traditional chemoradiotherapy (CRT) in 2020-2021. The primary endpoints were the pathologic complete response rate and the sustained clinical complete response rate in patients under W&W.
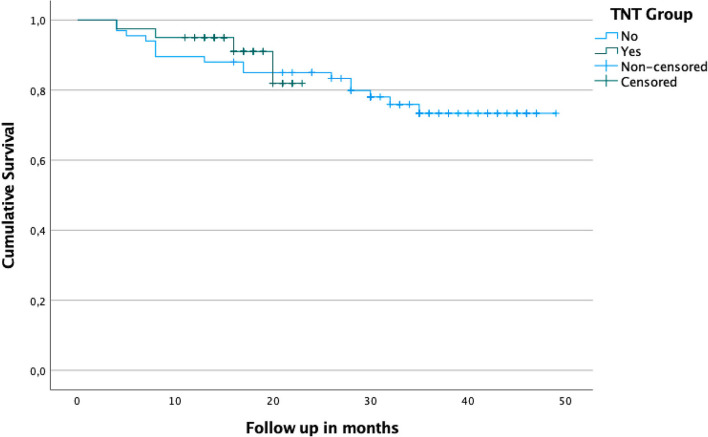
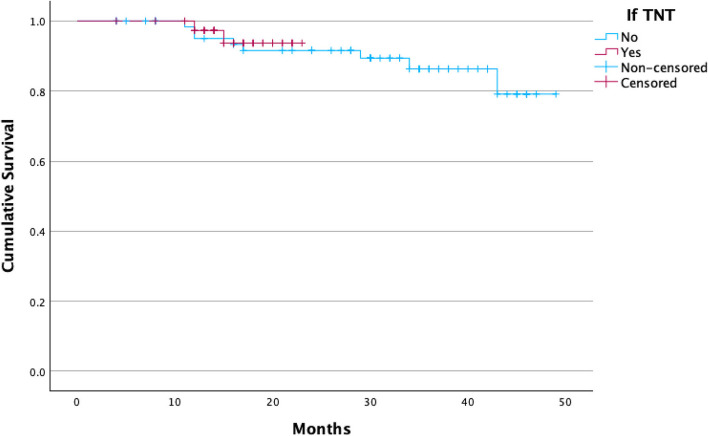
Results: Among 107 patients (54.2% male, mean age 62.48 years), non-TNT (67 patients) and TNT (40 patients) mean follow-ups were 26.7 and 8.2 months, respectively. No differences in gender(p = 0.163), staging (p = 0.707), or location (p = 0.727) were noted. TNT patients received more short-course radiotherapy (42.5% vs1.5%, p < 0.001). Clinical responses favored TNT (p = 0.030) with no significant differences in pathological responses, recurrence rates, or survival. TNT exhibited higher chemotherapy completion (p = 0.007) and lower adverse events (p < 0.001). Post-surgery events showed no significant differences (p = 0.470). Single center with retrospective design and carries limitations that may restrict the generalizability of the findings and the relatively short follow-up duration are our main limitations.
Conclusion: Our data add to the body of literature favoring the TNT treatment strategy for locally advanced rectal cancer, aiming to achieve comparable complete response rates with less adverse events.
Keywords: Adjuvant chemotherapy; Chemoradiotherapy; Complete clinical response; Locally advanced rectal cancer; Total neoadjuvant therapy; Treatment completion rates.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the local institutional Ethical Committee board (Comissão de Etica para a Saúde of Instituto Português de Oncologia de Lisboa Francisco Gentil, with the protocol code UIC/1649). Consent for publication: The manuscript does not contain any individual person’s data in any form, so inform consent is not necessary. Competing interests: The authors declare no competing interests.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021May;71(3):209–49. 10.3322/caac.21660. (Epub 2021 Feb 4 PMID: 33538338). - DOI - PubMed
-
- Maas M, Beets-Tan RG, Lambregts DM, Lammering G, Nelemans PJ, Engelen SM, van Dam RM, Jansen RL, Sosef M, Leijtens JW, Hulsewé KW, Buijsen J, Beets GL. Wait-and-see policy for clinical complete responders after chemoradiation for rectal cancer. J Clin Oncol. 2011D 10;29(35):4633–40. 10.1200/JCO.2011.37.7176. Epub 2011 Nov 7 PMID: 22067400. - DOI - PubMed
-
- van der Valk MJM, Hilling DE, Bastiaannet E, Meershoek-Klein Kranenbarg E, Beets GL, Figueiredo NL, Habr-Gama A, Perez RO, Renehan AG, van de Velde CJH; IWWD Consortium. Long-term outcomes of clinical complete responders after neoadjuvant treatment for rectal cancer in the International Watch & Wait Database (IWWD): an international multicentre registry study. Lancet. 2018 Jun 23;391(10139):2537–2545. 10.1016/S0140-6736(18)31078-X. PMID: 29976470. - PubMed
-
- Bahadoer RR, Dijkstra EA, van Etten B, Marijnen CAM, Putter H, Kranenbarg EM, Roodvoets AGH, Nagtegaal ID, Beets-Tan RGH, Blomqvist LK, Fokstuen T, Ten Tije AJ, Capdevila J, Hendriks MP, Edhemovic I, Cervantes A, Nilsson PJ, Glimelius B, van de Velde CJH, Hospers GAP; RAPIDO collaborative investigators. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): a randomised, open-label, phase 3 trial. Lancet Oncol. 2021 Jan;22(1):29–42. 10.1016/S1470-2045(20)30555-6. Epub 2020 Dec 7. Erratum in: Lancet Oncol. 2021 Feb;22(2):e42. PMID: 33301740.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
