

Feasibility of newly designed rotatable sphincterotome for endoscopic sphincterotomy (with video)
- PMID: 39610948
- PMCID: PMC11604308
- DOI: 10.1055/a-2422-2425
Feasibility of newly designed rotatable sphincterotome for endoscopic sphincterotomy (with video)
Erratum in
-
Correction: Feasibility of newly designed rotatable sphincterotome for endoscopic sphincterotomy (with video).Endosc Int Open. 2024 Dec 4;12(11):C11. doi: 10.1055/a-2494-7841. eCollection 2024 Nov. Endosc Int Open. 2024. PMID: 39635272 Free PMC article.
Abstract
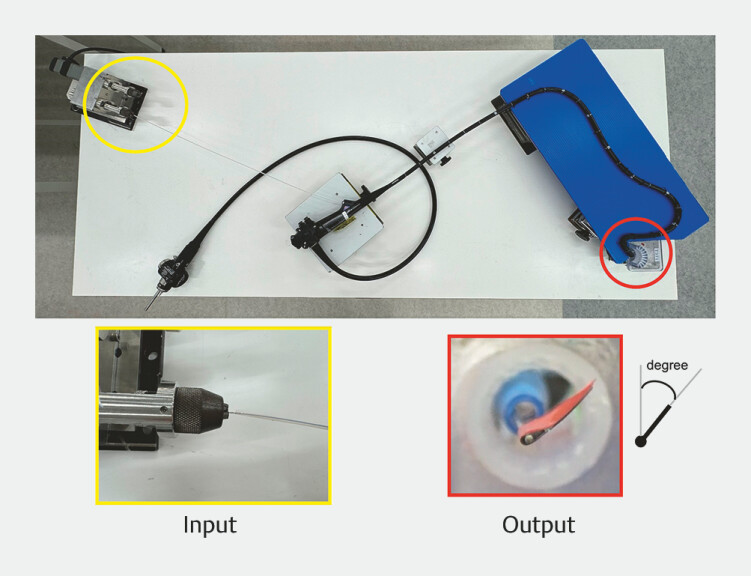
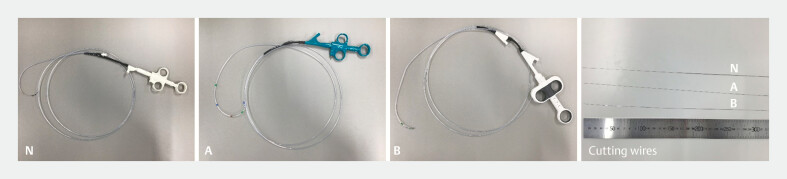
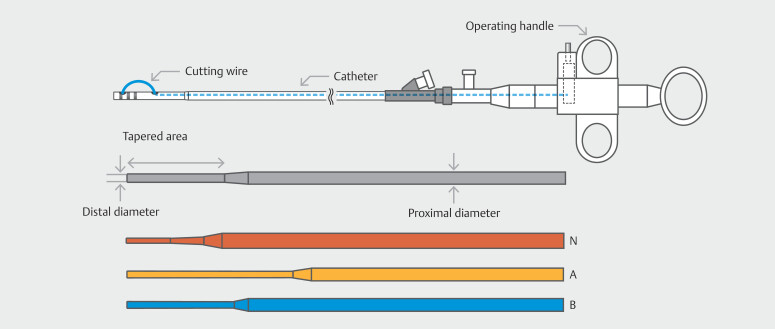
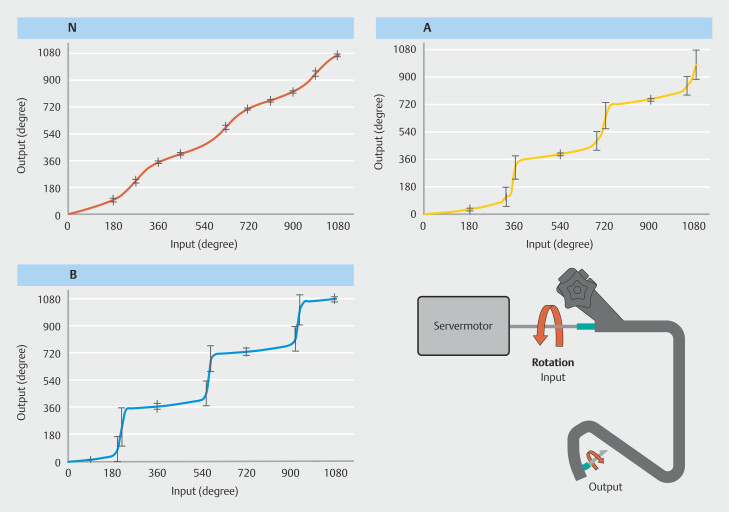
Background and study aims Endoscopic sphincterotomy can be challenging especially in patients with surgically altered anatomy. Although a rotatable sphincterotome (r-sphincterotome) may be useful, its rotational function is often inadequate. We evaluated the feasibility of a newly designed r-sphincterotome equipped with a well-conceived cutting wire. Methods We measured the movement and dynamics of both the newly designed r-sphincterotome and two existing r-sphincterotomes using in-house equipment. Ideally, the rotational force exerted at the proximal end should transmit directly to the distal end. But it is often challenging, particularly within the constraints of a bent endoscope and working channel. We collected data regarding deviation from the ideal value 10 times for each sphincterotome. Results The deviation from the ideal value was significantly lower with the newly designed r-sphincterotome than with the conventional r-sphincterotomes (44.9 ± 27.8 vs. 73.7 ± 44.6 and 130.1 ± 71.4 degrees, respectively; P < 0.001). The newly designed r-sphincterotome rotated smoothly and consistently at a constant speed, mirroring the input rotation. Conclusions We evaluated the feasibility of the newly designed r-sphincterotome using an experimental model. We believe that the findings from these experiments may contribute to easier and more precise sphincterotomies.
Keywords: ERC topics; Pancreatobiliary (ERCP/PTCD); Performance and complications; Quality and logistical aspects; Quality management; Training.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Conflict of Interest The authors declare that they have no conflict of interest.
Figures
References
-
- Kurita A, Kudo Y, Yoshimura K et al. Comparison between a rotatable sphincterotome and a conventional sphincterotome for selective bile duct cannulation. Endoscopy. 2019;51:852–857. - PubMed
-
- Bedogni G, Bertoni G, Contini S et al. Endoscopic sphincterotomy in patients with Billroth II partial gastrectomy: comparison of three different techniques. Gastrointest Endosc. 1984;30:300–304. - PubMed
-
- Shimatani M, Matsushita M, Takaoka M et al. Effective "short" double-balloon enteroscope for diagnostic and therapeutic ERCP in patients with altered gastrointestinal anatomy: a large case series. Endoscopy. 2009;41:849–854. - PubMed
-
- Hori Y, Naitoh I, Miyabe K et al. Simultaneous side-by-side bilateral metal stent placement using a colonoscope in a patient with Billroth II reconstruction. Endoscopy. 2018;50:E218–E219. - PubMed
LinkOut - more resources
Full Text Sources