

Unbiased immunome characterisation correlates with COVID-19 mRNA vaccine failure in immunocompromised adults
- PMID: 39611158
- PMCID: PMC11602488
- DOI: 10.3389/fimmu.2024.1405217
Unbiased immunome characterisation correlates with COVID-19 mRNA vaccine failure in immunocompromised adults
Abstract
Introduction: Coronavirus disease 2019 (COVID-19) affects the population unequally, with a greater impact on older and immunosuppressed people.
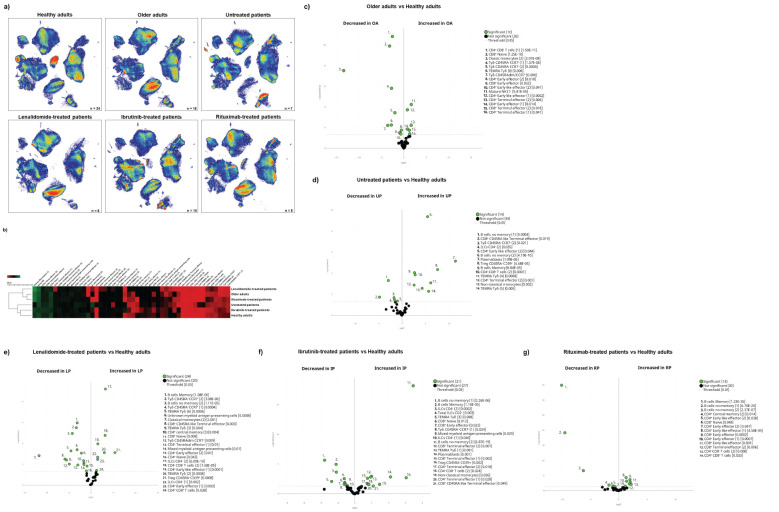
Methods: Hence, we performed a prospective experimental cohort study to characterise the effect of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccination in immune-compromised patients (older adults and oncohaematologic patients), compared with healthy counterparts, based on deep characterisation of the circulating immune cell subsets.
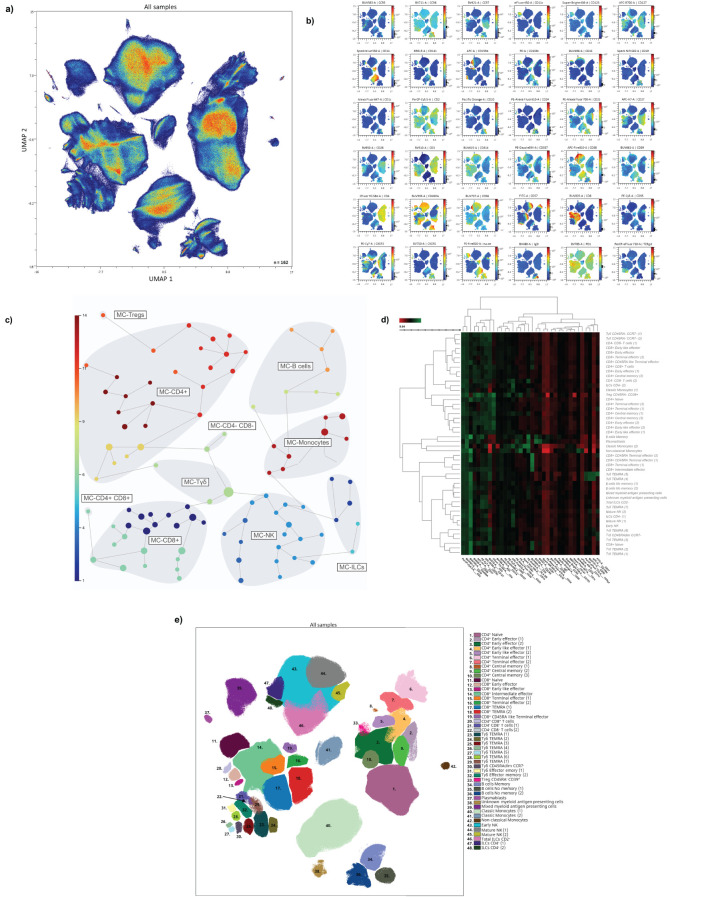
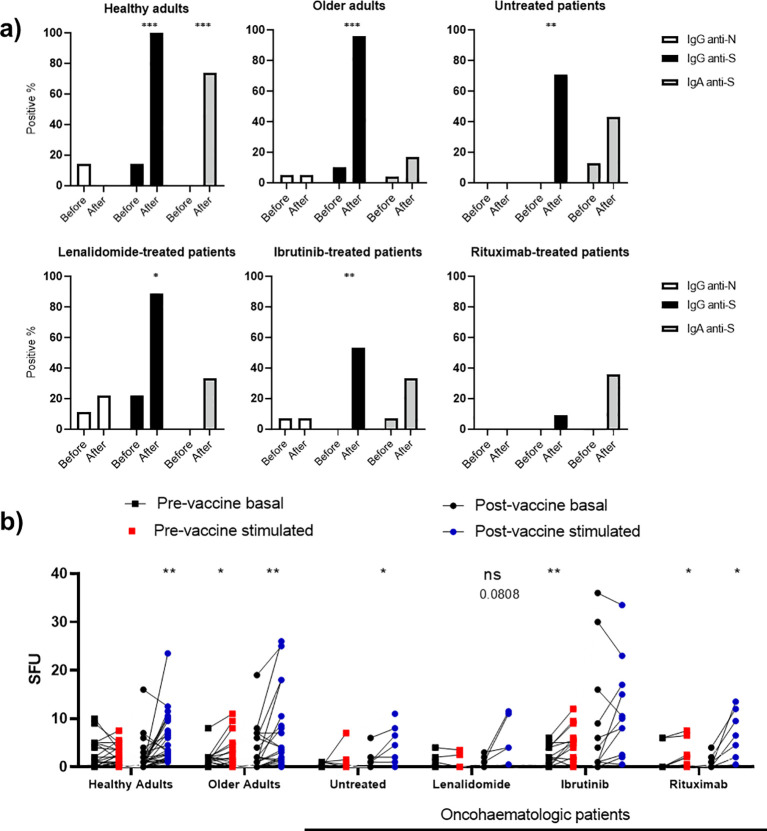
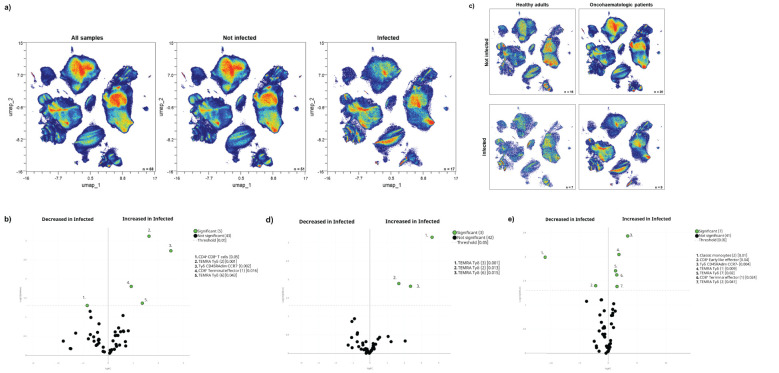
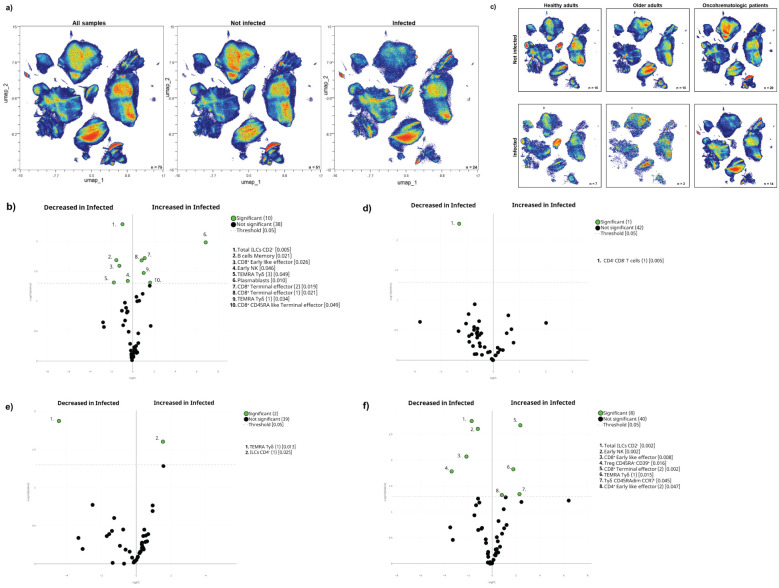
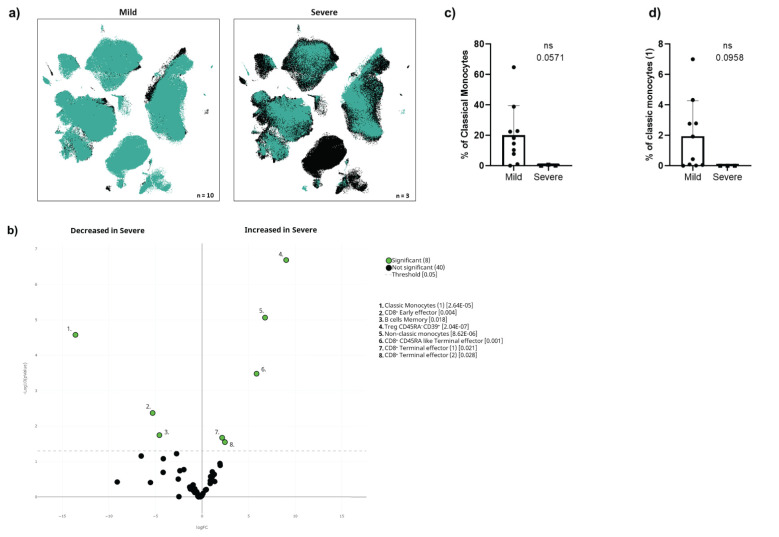
Results and discussion: While acquired humoral and cellular memory did not predict subsequent infection 18 months after full vaccination, spectral and computational cytometry revealed several subsets within the CD8+ T-cells, B-cells, natural killer (NK) cells, monocytes and TEMRA Tγδ cells that were differentially expressed in individuals who were subsequently infected and not infected not just following immunisation, but also prior to vaccination. Of note, we found up to seven clusters within the TEMRA Tγδ cell population, with some of them being expanded and others decreased in subsequently infected individuals. Moreover, some of these cellular clusters were also related to COVID-19-induced hospitalisation in oncohaematologic patients. Therefore, we have identified a cellular signature that even before vaccination is related to COVID-19 vulnerability as opposed to the acquisition of cellular and/or humoral memory following vaccination with SARS-CoV-2 messenger RNA (mRNA) vaccines.
Keywords: COVID-19; computational cytometry; immunocompromised adult; immunome; vaccine failure.
Copyright © 2024 H-Vázquez, Cal-Sabater, Arribas-Rodríguez, Fiz-López, Perez-Segurado, Martín-Muñoz, De Prado, Perez Mazzali, de Castro, del Hierro, de la Fuente Graciani, Pérez González, Gutiérrez, Tellería, Novoa, Rojo Rello, Garcia-Blesa, Sedano, Martínez García, Garcinuño Pérez, Domínguez-Gil, Hernán García, Guerra, Muñoz-Sánchez, Barragan-Pérez, Diez Morales, Casazza Donnarumma, Ramos Pollo, Santamarta Solla, Álvarez Manzanares, Bravo, García Alonso, Avendaño Fernández, Gay Alonso, Garrote, Arranz, Eiros, Rescalvo Santiago, Quevedo Villegas, Tamayo, Orduña, Dueñas, Peñarrubia, Cuesta-Sancho, Montoya and Bernardo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Rescigno M, Agrati C, Salvarani C, Giannarelli D, Costantini M, Mantovani A, et al. Neutralizing antibodies to Omicron after the fourth SARS-CoV-2 mRNA vaccine dose in immunocompromised patients highlight the need of additional boosters. Front Immunol. (2023) 14. doi: 10.3389/fimmu.2023.1104124 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous