

Spinal cord evaluation in multiple sclerosis: clinical and radiological associations, present and future
- PMID: 39611182
- PMCID: PMC11604059
- DOI: 10.1093/braincomms/fcae395
Spinal cord evaluation in multiple sclerosis: clinical and radiological associations, present and future
Abstract
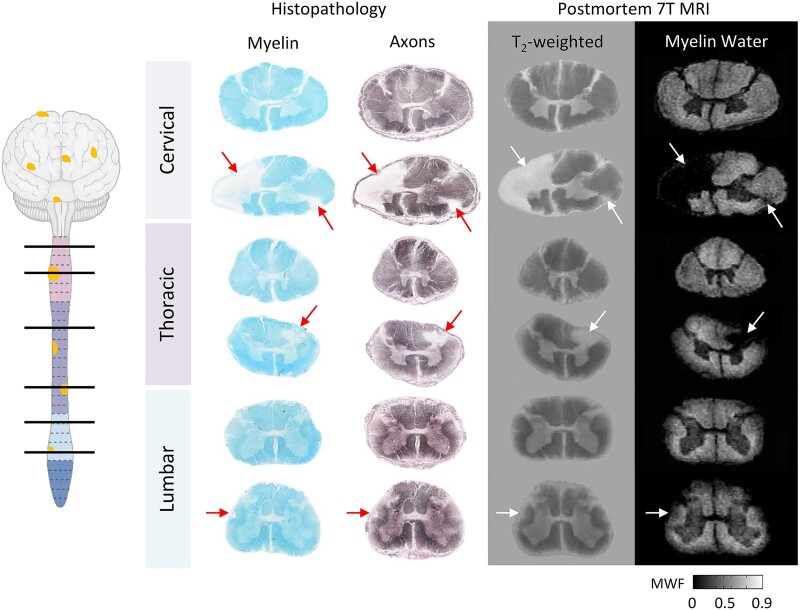
Spinal cord disease is important in most people with multiple sclerosis, but assessment remains less emphasized in patient care, basic and clinical research and therapeutic trials. The North American Imaging in Multiple Sclerosis Spinal Cord Interest Group was formed to determine and present the contemporary landscape of multiple sclerosis spinal cord evaluation, further existing and advanced spinal cord imaging techniques, and foster collaborative work. Important themes arose: (i) multiple sclerosis spinal cord lesions (differential diagnosis, association with clinical course); (ii) spinal cord radiological-pathological associations; (iii) 'critical' spinal cord lesions; (iv) multiple sclerosis topographical model; (v) spinal cord atrophy; and (vi) automated and special imaging techniques. Distinguishing multiple sclerosis from other myelopathic aetiology is increasingly refined by imaging and serological studies. Post-mortem spinal cord findings and MRI pathological correlative studies demonstrate MRI's high sensitivity in detecting microstructural demyelination and axonal loss. Spinal leptomeninges include immune inflammatory infiltrates, some in B-cell lymphoid-like structures. 'Critical' demyelinating lesions along spinal cord corticospinal tracts are anatomically consistent with and may be disproportionately associated with motor progression. Multiple sclerosis topographical model implicates the spinal cord as an area where threshold impairment associates with multiple sclerosis disability. Progressive spinal cord atrophy and 'silent' multiple sclerosis progression may be emerging as an important multiple sclerosis prognostic biomarker. Manual atrophy assessment is complicated by rater bias, while automation (e.g. Spinal Cord Toolbox), and artificial intelligence may reduce this. Collaborative research by the North American Imaging in Multiple Sclerosis and similar groups with experts combining distinct strengths is key to advancing assessment and treatment of people with multiple sclerosis spinal cord disease.
Keywords: atrophy; magnetic resonance imaging; multiple sclerosis; pathology; spinal cord.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
B.M.K.: consulting EMD Serono, royalties Oxford University Press Mayo Clinic Cases in Neuroimmunology. M.A.: consulting Biogen, Abata Therapeutics, Sanofi-Genzyme and GSK. E.P.F.: grants or contracts UCB, NIH and Medimmune/Viela Bio/Horizon Therapeutics; royalties UpToDate; honoraria Pharmacy Times; Patents DACH1-IgG as a biomarker of paraneoplastic autoimmunity; participation on a Data Safety Monitoring Board Alexion, Genentech, Horizon Therapeutics and UCB, MOG project; and leadership or fiduciary roles Journal of the Neurological Sciences and Neuroimmunology Reports. R.G.H.: grants or contracts Roche/Genentech and Atara; consulting Roche/Genentech Boston Pharma QIA and LLC; honoraria Sanofi; and participation on a Data Safety Monitoring Board Roche and Novartis. E.C.K: grants or contracts AbbVie, Biogen, Genentech; consulting Banner Life Sciences, EMD Serono, Galen/Atlantica Genentech, Greenwich Biosciences, INmune Bio, Myrobalan Therapeutics, OM1 and TG Therapeutics, honoraria BioPharm Communications, MJH Lifesciences; and participation on a Data Safety Monitoring Board Tiziana Life Sciences. S.K: grants Roche and Biogen. S.K.: grants or contracts Biogen BMS Novartis Sanofi; consulting Baim Institute Biogen Cycle EMD Serono Genentech Novartis Ootave Genzyme/Sanofi TG Therapeutics; and honoraria Biogen EMD Serono Genentech TG Therapeutics. N.P.: research support Race to Erase MS. A.T.: grants or contracts Hilton Foundation, Roche, AbbVie, honoraria Biogen and Roche, support for attending meetings EMD Serono; and participation on a Data Safety Monitoring Board Sanofi Genzyme, Roche. J.C.-A., C.L., J.A.L., S.M., J.O. and S.A.S.: no competing interests.
Figures




References
-
- Thompson AJ, Banwell BL, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018;17(2):162–173. - PubMed
-
- Laule C, Yung A, Pavolva V, et al. High-resolution myelin water imaging in post-mortem multiple sclerosis spinal cord: A case report. Mult Scler. 2016;22(11):1485–1489. - PubMed
Publication types
LinkOut - more resources
Full Text Sources