

Implementation of a crash cesarean section policy and its impact on maternal and neonatal outcomes at King Abdulaziz University Hospital: A retrospective study
- PMID: 39612466
- PMCID: PMC11608669
- DOI: 10.1097/MD.0000000000040645
Implementation of a crash cesarean section policy and its impact on maternal and neonatal outcomes at King Abdulaziz University Hospital: A retrospective study
Abstract
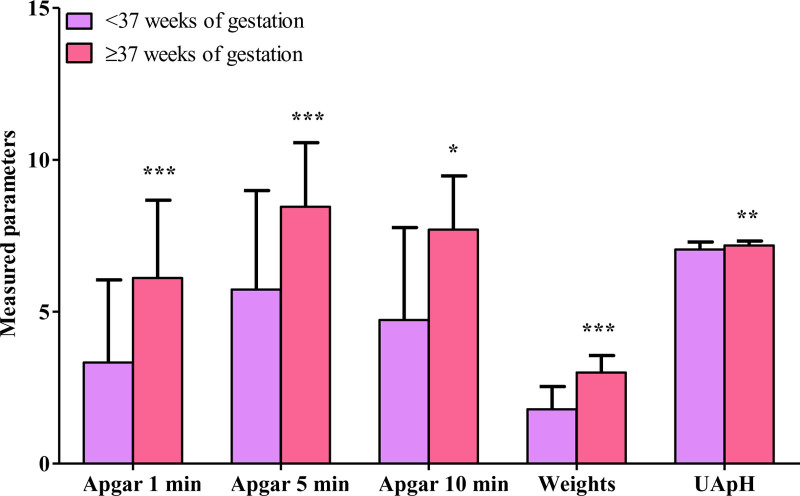
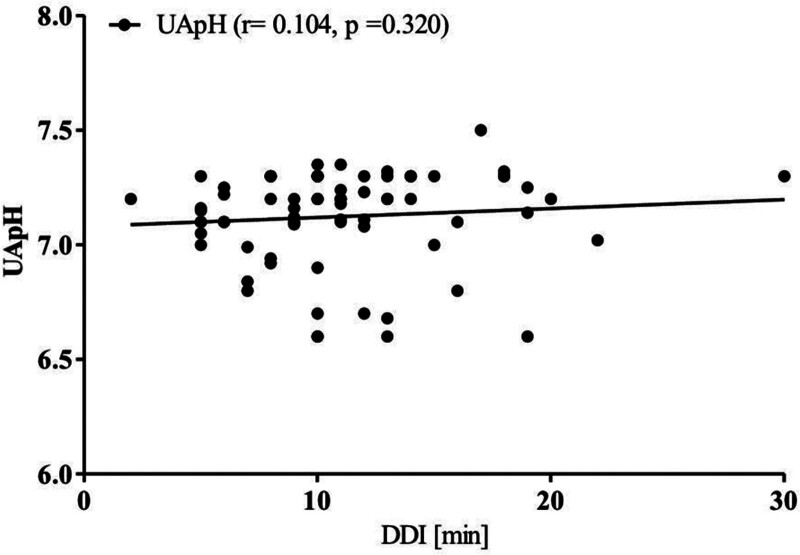
A typical surgical technique for pregnant women with potentially fatal problems affecting the mother or fetus is an emergency cesarean section (ECS). The decision-to-delivery interval (DDI) for ECS should be within 30 minutes. The objective of this study was to investigate crash ECS indications and effects on maternal and neonatal outcomes. In this retrospective study, all women undergoing crash cesarean section (CS) at Obstetrics and Gynecology department at King Abdulaziz University hospital, Jeddah, Saudi Arabia during 2022 and 2023 were evaluated. Data about demographic and obstetric characteristics of mother, ECS indications, DDI, and outcomes for mothers and newborns was gathered from the patient's sheet. One hundred 3 crash CS were performed during study period. Crash CS indications were fetal bradycardia (64.1%), prolapsed cord (24.3%), uterine rupture (6.8%), and severe antepartum hemorrhage (4.9%). D-D time range from 2 to 30 minutes. DDI was ≤15 minutes in 90 patients (87.4%) and >15 minutes in 13 patients (12.6%). Gestational age was <32 weeks (16.7%), between 32 and <37 weeks (15.5%), and ≥37 weeks (68.0%). Good maternal outcome was reported in 89 (86.4%), while 24 (13.6%) had complications. Intensive care unit maternal admission was significantly higher in gestational age 32 to <37 weeks versus <32 weeks and ≥37 weeks of gestation (18.8% vs 5.9% and 2.9%, P = .050). Fetal outcome was good in 69 (67.0%), while 34 (33.0%) had complications. Neonatal body weights, Apgar score at 1, 5, 10 minutes, and umbilical cord arterial pH were significantly decreased in preterm versus termed neonates (P < .0001, P < .0001, P < .0001, P = .014, and P = .003). Moreover, respiratory distress syndrome, jaundice, intubation, neonatal deaths, and sepsis were significantly higher in preterm versus term deliveries (P < .0001, P = .029, P < .0001, P = .010, and P = .031). Good neonatal outcome was significantly higher (P < .0001); while respiratory distress syndrome was significantly lower (P = .007) in deliveries with DDI ≤ 15 minutes versus > 15 minutes. The 30-minute standard for DDI time interval may be a feasible guideline at least for level-3 hospitals. Crash CS indication was mostly due to fetal bradycardia. The maternal and neonatal outcomes were better in term than preterm deliveries. The positive effect of very short intervals on neonatal outcome still needs to be proven.
Copyright © 2024 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
Maternal and Neonatal Outcomes among Obese Pregnant Women in King Abdulaziz University Hospital: A Retrospective Single-Center Medical Record Review.Med Arch. 2019 Dec;73(6):425-432. doi: 10.5455/medarh.2019.73.425-432. Med Arch. 2019. PMID: 32082014 Free PMC article.
-
Crash emergency cesarean section: decision-to-delivery interval under 30 min and its effect on Apgar and umbilical artery pH.Arch Gynecol Obstet. 2005 Dec;273(3):161-5. doi: 10.1007/s00404-005-0045-7. Epub 2005 Jul 26. Arch Gynecol Obstet. 2005. PMID: 16044190
-
The impact of cesarean section on neonatal outcomes at a university-based tertiary hospital in Jordan.BMC Pregnancy Childbirth. 2020 Jun 1;20(1):335. doi: 10.1186/s12884-020-03027-2. BMC Pregnancy Childbirth. 2020. PMID: 32487165 Free PMC article.
-
Emergency delivery in pregnancies at high probability of placenta accreta spectrum on prenatal imaging: a systematic review and meta-analysis.Am J Obstet Gynecol MFM. 2024 Oct;6(10):101432. doi: 10.1016/j.ajogmf.2024.101432. Epub 2024 Jul 26. Am J Obstet Gynecol MFM. 2024. PMID: 39069207
-
Effects of induction of labor prior to post-term in low-risk pregnancies: a systematic review.JBI Database System Rev Implement Rep. 2019 Feb;17(2):170-208. doi: 10.11124/JBISRIR-2017-003587. JBI Database System Rev Implement Rep. 2019. PMID: 30299344 Free PMC article.
References
-
- Lagrew DC, Bush MC, McKeown AM, Lagrew NG. Emergent (crash) cesarean delivery: indications and outcomes. Am J Obstet Gynecol. 2006;194:1638–43; discussion 1643. - PubMed
-
- Soltanifar S, Russell R. The National Institute for Health and Clinical Excellence (NICE) guidelines for caesarean section, 2011 update: implications for the anaesthetist. Int J Obstet Anesth. 2012;21:264–72. - PubMed
-
- Radhakrishnan G, Yadav G, Vaid NB, Ali H. Factors affecting“ decision to delivery interval” in emergency caesarean sections in a tertiary care hospital: a cross sectional observational study. Int J Reprod Contracept Obstet Gynecol. 2013;2:651–7.
-
- American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 487: preparing for clinical emergencies in obstetrics and gynecology. Obstet Gynecol. 2011;117:1032–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
