

Investigating the effect of verapamil on preservation of beta-cell function in adults with newly diagnosed type 1 diabetes mellitus (Ver-A-T1D): protocol for a randomised, double-blind, placebo-controlled, parallel-group, multicentre trial
- PMID: 39613428
- PMCID: PMC11605811
- DOI: 10.1136/bmjopen-2024-091597
Investigating the effect of verapamil on preservation of beta-cell function in adults with newly diagnosed type 1 diabetes mellitus (Ver-A-T1D): protocol for a randomised, double-blind, placebo-controlled, parallel-group, multicentre trial
Abstract
Introduction: Type 1 diabetes mellitus (T1DM) is a disorder that arises following the selective autoimmune destruction of the insulin-producing beta cells. Beta-cell protective or beta-cell regenerative approaches have gained wider attention, and pharmacological approaches to protect the patient's own insulin-producing beta-cell mass have been proposed. Verapamil is an L-type calcium channel blocker that has been reported to effectively lowers beta-cell thioredoxin-interacting protein expression in rodent beta cells and islets, as well as in human islets, and thus promotes functional beta-cell mass.
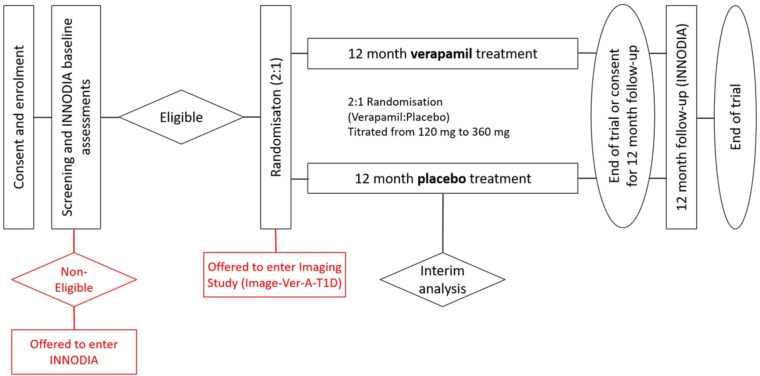
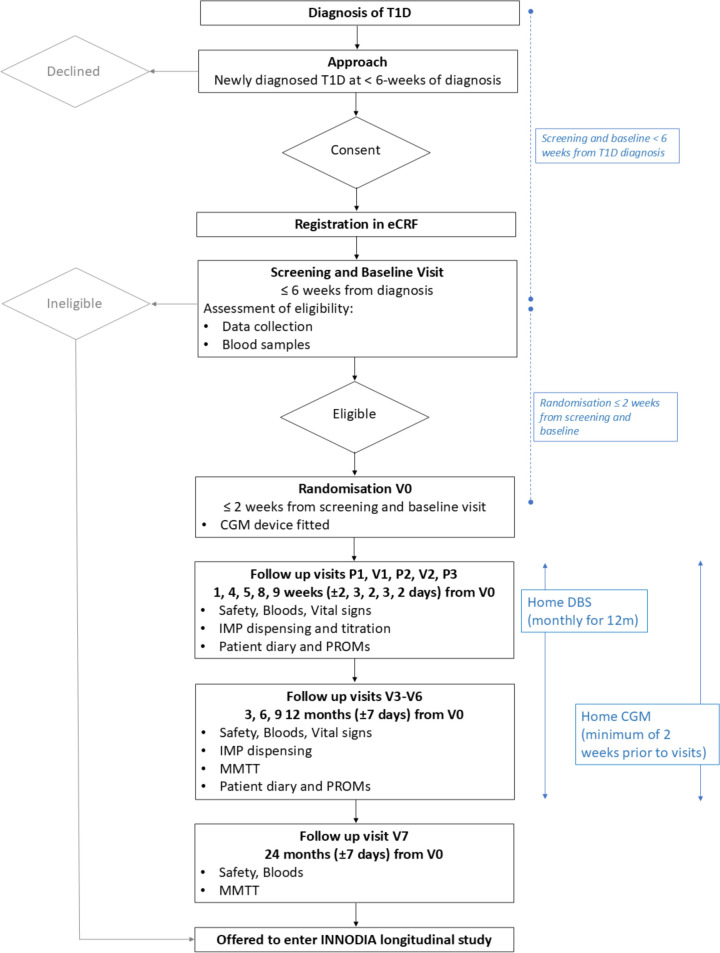
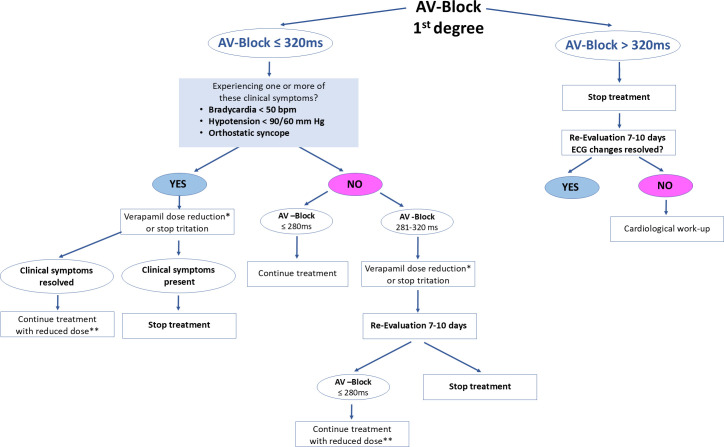
Methods and analysis: The trial is a multicentre, randomised, double-blind, placebo-controlled trial in participants with T1DM, investigating the effect of verapamil on preservation of beta-cell function (Ver-A-T1D). A total of 120 participants will be randomised in a 2:1 ratio between 360 mg verapamil and placebo, administered orally once daily. T1DM patients aged ≥18 and <45 years will be eligible for recruitment within 6 weeks of diagnosis (defined as day of starting insulin therapy). The primary objective will be to determine the changes in stimulated C-peptide response during the first 2 hours of a mixed meal tolerance test at baseline and after 12 months for 360 mg verapamil administered orally once daily versus placebo. Secondary objectives include the effects of 360 mg verapamil on (1) fasting C-peptide, (2) dried blood spot C-peptide, (3) glycated haemoglobin, (4) daily total insulin dose, (5) time in range by intermittent continuous glucose monitoring measures, (6) other biomarkers related to immunological changes and beta-cell death and (6) safety (vital signs, ECG).
Ethics and dissemination: Ethics approval was sought from the research ethics committee of all participating countries. All participants provided written informed consent before joining the study. Ver-A-T1D received first regulatory and ethical approvals in Austria. The publication policy is set in the innovative approach towards understanding and arresting type 1 diabetes grant agreement (www.innodia.eu).
Trial registration number: EudraCT, 2020-000435-45; ClinicalTrials.gov, NCT04545151.
Protocol version: Version 8.0 (08 November 2021).
Keywords: Clinical Trial; DIABETES & ENDOCRINOLOGY; Randomized Controlled Trial.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Diabetes Control and Complications Trial Research Group. Nathan DM, Genuth S, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–86. doi: 10.1056/NEJM199309303291401. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical