

Complete resection of a giant costal chondrosarcoma with reconstruction of the thoraco-abdominal wall: a case report
- PMID: 39614304
- PMCID: PMC11607819
- DOI: 10.1186/s13019-024-03145-4
Complete resection of a giant costal chondrosarcoma with reconstruction of the thoraco-abdominal wall: a case report
Abstract
Background: Chondrosarcoma primarily occurs in the pelvis and femur, with occasional cases in the ribs. Surgical resection remains the main treatment method for costal chondrosarcoma. However, complete resection often leads to a large range of chest wall defects and a challenging reconstruction.
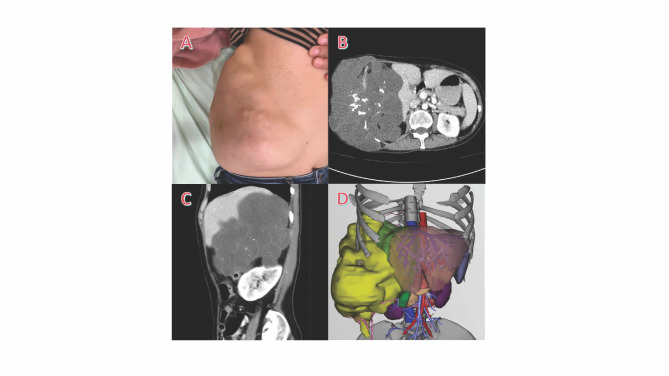
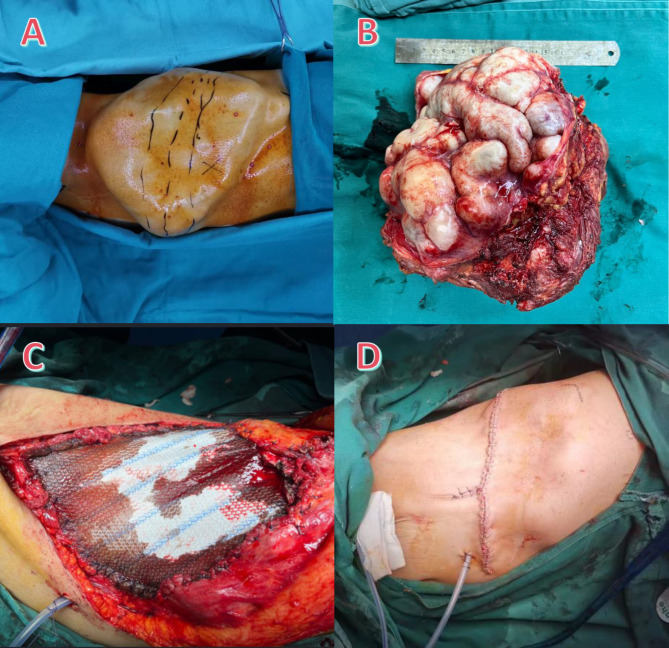
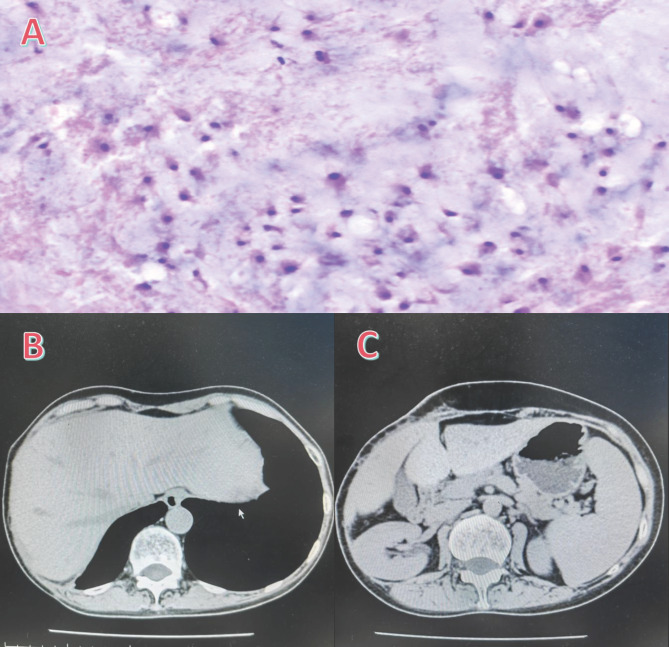
Case presentation: A 49-year-old female patient presented with progressive swelling of the right chest and abdominal wall over 15 years. Chest CT revealed a 20.1 × 15.6 × 13.7 cm multilocular cystic-solid mass with internal calcification, encircling the 8th to 12th ribs and causing elevation of the right diaphragm. Compression of the liver resulting in a significant reduction in volume. Based on an ultrasound-guided biopsy, chondrosarcoma Grade I was diagnosed. After a multi-disciplinary discussion, we performed a complete resection of the tumor, including the 8th to 12th anterolateral ribs and part of the diaphragm. The diaphragm was then reconstructed by suturing it to the ribs and intercostal muscles at the resection margin. The thoraco-abdominal wall defects were reconstructed with a polypropylene mesh. Finally, we excised the excess skin and then closed the incision. Histopathologic diagnosis was chondrosarcoma Grade II. The postoperative course was uneventful. At the 3-month postoperative follow-up, no signs of recurrence were observed.
Conclusions: Wide en-bloc resection followed by reconstruction using polypropylene mesh is feasible and cost-effective for costal chondrosarcoma with limited invasion. This case illustrates the importance of meticulous preoperative planning and multi-disciplinary discussion.
Keywords: Case report; Chondrosarcoma; Reconstruction; Thoraco-abdominal wall.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Our study was approved by the Ethics Committee for Medical Research and New Medical Technology of Sichuan Cancer Hospital (No. SCCHEC-02-2024-138). Consent for publication: Informed consent for publication was obtained. Competing interests: The authors declare no competing interests.
Figures
References
-
- Al-Refaie RE, Amer S, Ismail MF, et al. Chondrosarcoma of the chest wall: single-center experience. Asian Cardiovasc Thorac Ann. 2014;22(7):829–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
