

Intra-aortic balloon pump after VA-ECMO reduces mortality in patients with cardiogenic shock: an analysis of the Chinese extracorporeal life support registry
- PMID: 39614333
- PMCID: PMC11606124
- DOI: 10.1186/s13054-024-05129-1
Intra-aortic balloon pump after VA-ECMO reduces mortality in patients with cardiogenic shock: an analysis of the Chinese extracorporeal life support registry
Abstract
Background: The role of intra-aortic balloon pump (IABP) combined with venoarterial extracorporeal membrane oxygenation (VA-ECMO) in patients with cardiogenic shock (CS) remains unclear. This study investigated the effect of applying IABP for left ventricle (LV) unloading after VA-ECMO on reducing mortality in patients with CS.
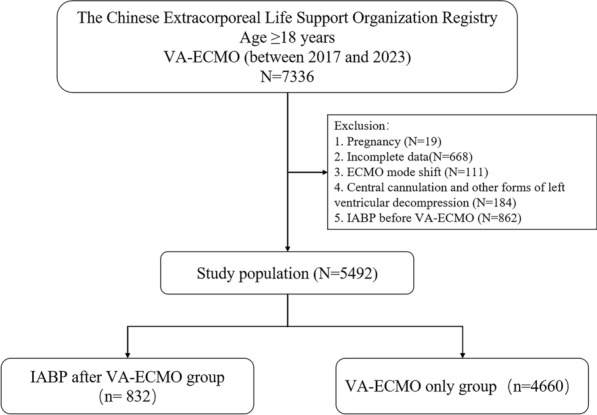
Methods: Data from 5,492 consecutive patients with CS treated with VA-ECMO between January 2017 and July 2023 were collected from the CSECLS registry. The primary outcome was in-hospital mortality. The secondary outcomes included 30-day mortality, survival on VA-ECMO, and various complications. The association between the application of IABP after VA-ECMO and in-hospital outcomes was assessed.
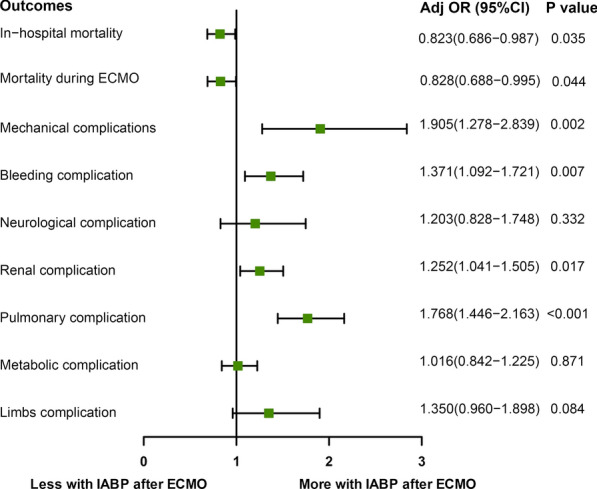
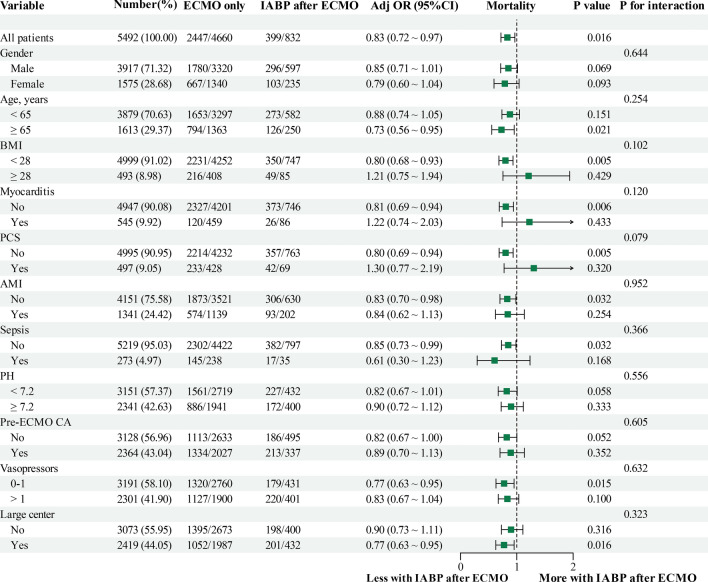
Results: Among 5,492 patients undergoing VA-ECMO (mean age 54.7 ± 15.1 years, 3,917 [71.3%] male), 832 (15.1%) received IABP after VA-ECMO. Before VA-ECMO, a higher incidence of cardiac intervention (13.9% vs. 16.7%) and myocardial infarction (12.0% vs. 14.8%) (all P < 0.05) was seen in the IABP after VA-ECMO group. In this cohort, the IABP after VA-ECMO group had a lower in-hospital mortality (52.5% vs. 48.0%, P = 0.017) and a higher survival rate on VA-ECMO (75.4% vs. 79.4%, P = 0.014). On multivariate modeling, the use of IABP after VA-ECMO was associated with a lower risk of in-hospital mortality (adjusted odds ratio[aOR], 0.823 [95% confidence interval [CI], 0.686-0.987]; P = 0.035) and on-support mortality (aOR, 0.828 [95% CI, 0.688-0.995]; P = 0.044). However, the use of IABP after VA-ECMO was also associated with an increased incidence of complications, including mechanical (aOR: 1.905, [95% CI, 1.278-2.839]; P = 0.002), bleeding (aOR: 1.371, [95% CI, 1.092-1.721]; P = 0.007), renal (aOR: 1.252, [95% CI, 1.041-1.505]; P = 0.017), and pulmonary (aOR: 1.768, [95% CI, 1.446-2.163]; P < 0.001).
Conclusion: In this multicenter retrospective study, the use of IABP after VA-ECMO was associated with lower in-hospital mortality in patients with CS. These findings suggest that IABP may offer advantages for LV unloading in patients with CS treated with VA-ECMO, but further validation through randomized controlled trials is warranted to better understand the balance of risks and benefits.
Keywords: Cardiogenic shock; Intra-aortic balloon pump; Venoarterial extracorporeal membrane oxygenation.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the institutional ethics committee/review board of the Beijing Anzhen Hospital. Informed consent for demographic, physiological and hospital-outcome data analyses was not obtained because this observational study did not modify existing diagnostic or therapeutic strategies. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Becher PM, Schrage B, Sinning CR, Schmack B, Fluschnik N, Schwarzl M, et al. Venoarterial extracorporeal membrane oxygenation for cardiopulmonary support. Circulation. 2018;138(20):2298–300. 10.1161/CIRCULATIONAHA.118.036691. - PubMed
-
- Thiele H, Ohman EM, de Waha-Thiele S, Zeymer U, Desch S. Management of cardiogenic shock complicating myocardial infarction: an update 2019. Eur Heart J. 2019;40(32):2671–83. 10.1093/eurheartj/ehz363. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the european society of cardiology (ESC)developed with the special contribution of the heart failure association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–200. 10.1093/eurheartj/ehw128. - PubMed
-
- de Waha S, Desch S, Eitel I, Fuernau G, Lurz P, Sandri M, et al. Intra-aortic balloon counterpulsation—basic principles and clinical evidence. Vascul Pharmacol. 2014;60(2):52–6. 10.1016/j.vph.2013.12.003. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
