

Differential effects of thiamine and ascorbic acid in clusters of septic patients identified by latent variable analysis
- PMID: 39614357
- PMCID: PMC11606082
- DOI: 10.1186/s13054-024-05188-4
Differential effects of thiamine and ascorbic acid in clusters of septic patients identified by latent variable analysis
Abstract
Background: Thiamine and ascorbic acid have been proposed to mitigate the devastating consequences of sepsis and septic shock. To date, randomized controlled trials have failed to demonstrate a benefit of these therapies and heterogeneity of treatment effect is suspected. In this study, we aimed at assessing the heterogeneity of treatment effect of thiamine (B1) and the combination of B1 plus ascorbic acid (AA + B1) in critically ill patients with sepsis.
Methods: We conducted a bi-centric retrospective cohort study. All adult patients admitted to the ICU with sepsis or septic shock between January 2012 and August 2022 were included. Patient clusters were identified using latent variable analysis based on demographics and physiological variables obtained within 24 h of admission. Within each cluster and using inverse probability weighted Cox models, we compared in-hospital mortality between patients who received standard treatment (control), standard treatment plus B1 (B1 group), and standard treatment plus a combination of thiamine and ascorbic acid (AA + B1 group).
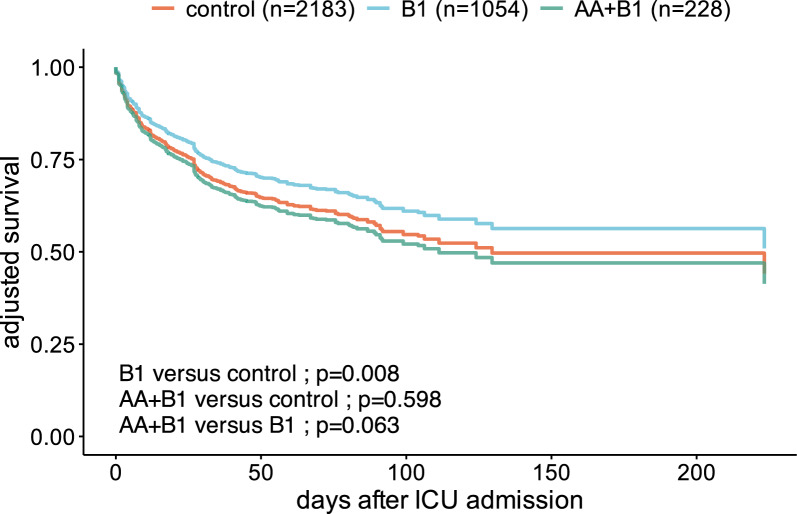
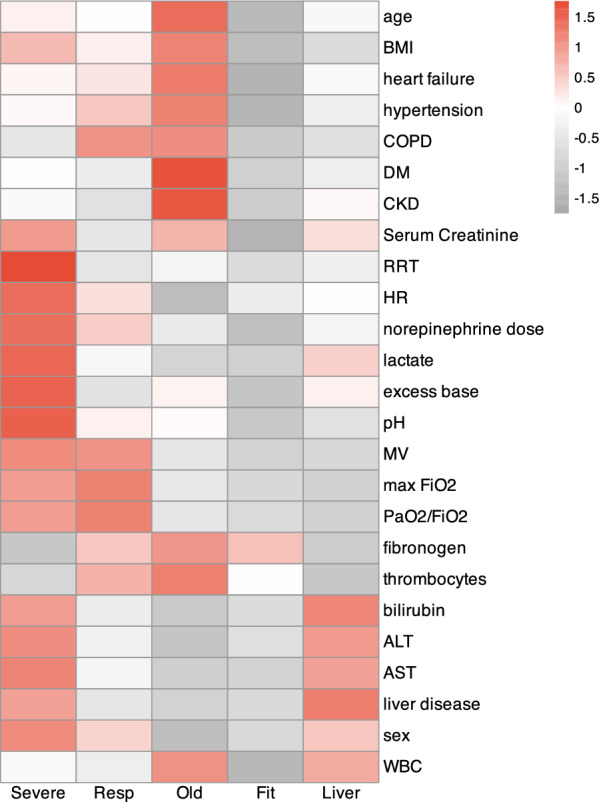
Results: A total of 3465 septic patients were included, 2183, 1054 and 228 in the standard, B1 and AA + B1 groups respectively. Five clusters of patients were identified in an unsupervised manner. The "Cluster Severe" included the most severely ill patients, the "Cluster Resp" patients presented with predominantly respiratory failure, the "Cluster Old" included elderly patients with multiple comorbidities, the "Cluster Fit" patients were young, healthy with low severity indices and "Cluster Liver" included patients with predominant liver failure. B1 treatment was associated with different outcomes across the five clusters. It was associated with a lower in-hospital mortality in the "Cluster Severe" and "Cluster Resp". On the other hand, the combination of thiamine and ascorbic acid was not associated with reduced mortality in any cluster but an increased mortality in"Cluster Old".
Conclusions: These results reinforce the lack of efficacy of the combination of AA + B1 reported in recent trials and even raise concerns about potential harm in older patients with comorbidities. On the contrary, we reported improved ICU survival associated with B1 supplementation in the most severe patients and those with predominant respiratory failure, supporting the need for further trials in this specific population.
Keywords: Ascorbic acid; HAT therapy; Sepsis; Thiamine.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the local ethical committee for human studies of Geneva, Switzerland (CCER 2023-00147, Commission Cantonale d’Ethique de la Recherche). The study was performed according to the Declaration of Helsinki principles. Consent for publication: All authors have approved the manuscript for submission. Competing interests: The authors declare no competing interests.
Figures

References
-
- Vincent J-L, Sakr Y, Sprung CL, et al. Sepsis in European intensive care units: results of the SOAP study. Crit Care Med. 2006;34(2):344–53. - PubMed
-
- Xie J, Wang H, Kang Y, et al. The epidemiology of sepsis in chinese ICUs: a national cross-sectional survey. Crit Care Med. 2020;48(3):e209–18. - PubMed
-
- Vincent J-L, Marshall JC, Namendys-Silva SA, et al. Assessment of the worldwide burden of critical illness: the intensive care over nations (ICON) audit. Lancet Respir Med. 2014;2(5):380–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
