

Management Challenges in Trauma-Induced Coagulopathy: A Case Report of Hemothorax Requiring Reoperation
- PMID: 39614607
- PMCID: PMC11613780
- DOI: 10.12659/AJCR.944997
Management Challenges in Trauma-Induced Coagulopathy: A Case Report of Hemothorax Requiring Reoperation
Abstract
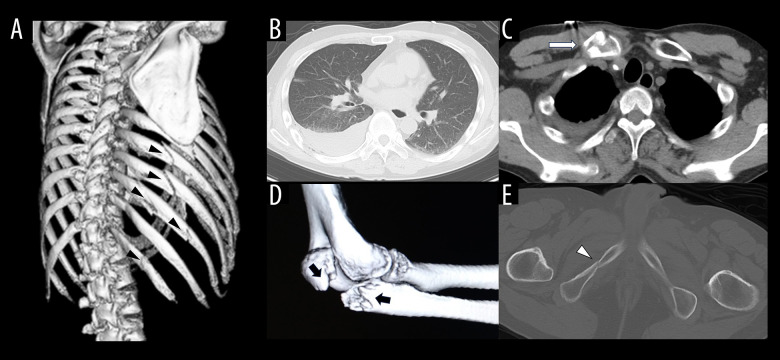
BACKGROUND Coagulopathy caused by trauma itself is defined as trauma-induced coagulopathy (TIC). The pathophysiology of TIC is considered to consist of coagulation activation, hyperfibrinolysis, and consumption coagulopathy, similar to disseminated intravascular coagulation (DIC). This report describes a 68-year-old man with a history of epilepsy presenting with TIC associated with multiple traumatic fractures and hemothorax. CASE REPORT A 68-year-old man with a history of epilepsy fell while working on a second-floor roof and had right rib fractures (6th to 12th rib), right hemothorax, right clavicle fracture, right elbow fracture, and pelvic fractures. The right hemothorax became exacerbated and he went into shock. We performed the emergency surgery 5 hours after the trauma. Although circulation dynamics became stable and the discharge of chest drainage became thinned at postoperative day (POD) 1 while administering blood transfusions and tranexamic acid, hemoglobin remained below 8 g/dl, platelet count was below 60 000/µl, and prothrombin time - international normalized ratio (1.22) remained prolonged. Furthermore, the right hemothorax became exacerbated and re-operation was performed on the evening of POD2. Oozing hemorrhages from multiple rib fractures were observed. Although hemostatic management was performed with electrocautery and ultrasound energy devices, the hemorrhage could not be completely managed, so hemostasis was secured using hemostatic materials. CONCLUSIONS The pathophysiologic mechanism of TIC has been emphasized as being different from that of DIC, and management of severe traumatic patients with TIC should be based on an understanding of the pathophysiology of TIC.
Conflict of interest statement
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
