

Relevance of Neutralizing Antibodies for the Pharmacokinetics of Pegunigalsidase Alfa in Patients with Fabry Disease
- PMID: 39614966
- PMCID: PMC11750932
- DOI: 10.1007/s40259-024-00690-1
Relevance of Neutralizing Antibodies for the Pharmacokinetics of Pegunigalsidase Alfa in Patients with Fabry Disease
Abstract
Background: Pegunigalsidase alfa is a newly approved drug for the treatment of Fabry disease, designed to increase the plasma half-life and reduce immunogenicity of infused α-galactosidase A (AGAL). We provide the first comprehensive pharmacokinetic and immunogenic data apart from industry-initiated studies.
Methods: Pharmacokinetics of pegunigalsidase alfa, amino acid, and polyethylene glycol (PEG)-specific antibodies and immune complexes were measured in treated patients (11 switched, two naïve). Measurements were performed in serum samples drawn directly before and after infusions over three to ten consecutive infusions. Only three patients started directly with 1.0 mg/kg body weight.
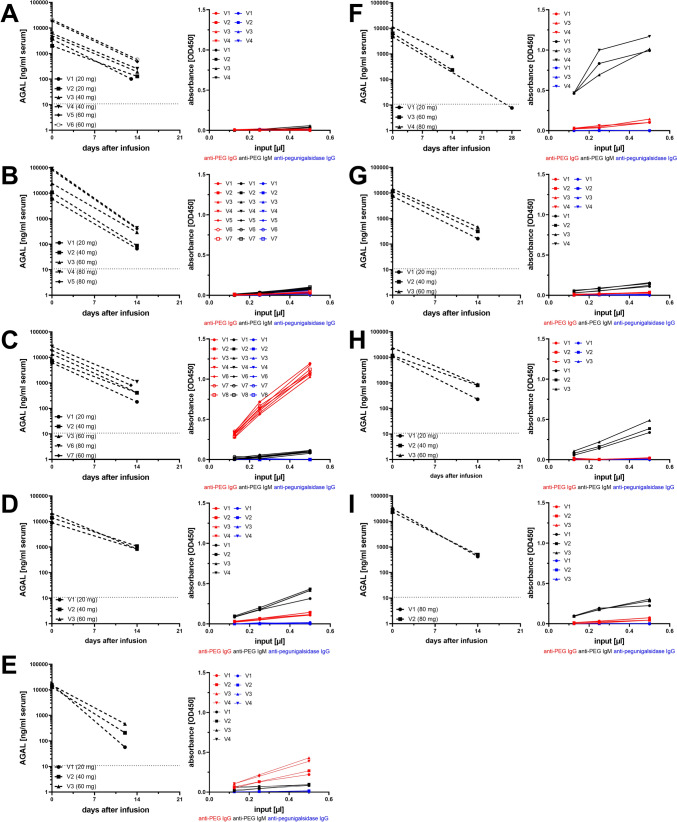
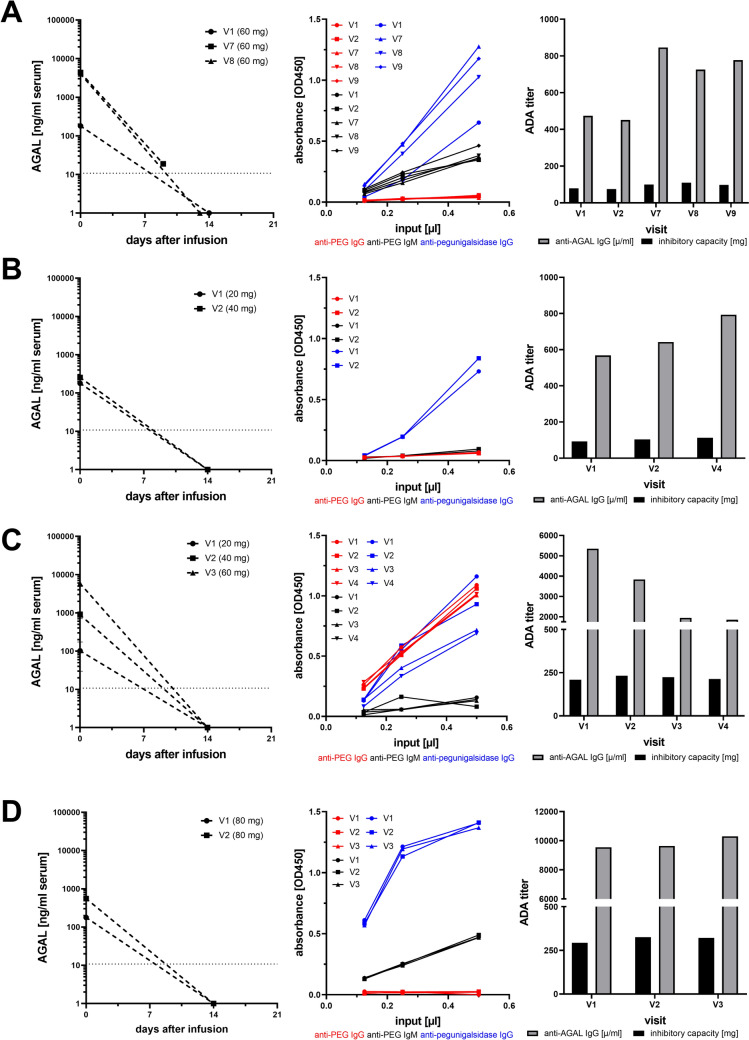
Results: No infusion-associated reactions were reported under pegunigalsidase alfa during the observation. Patients without pre-existing neutralizing anti-AGAL antibodies showed high enzymatic AGAL peak activities and sustained AGAL serum concentrations until the next infusion, which was not observed in those with neutralizing anti-AGAL antibodies. Nine (69.2%) patients presented with pre-existing anti-PEG antibodies (IgG or IgM), which seemed to have no impact on pharmacokinetics during the observation. No new anti-PEG or anti-AGAL antibody formation was observed after treatment initiation. Three (75.0%) patients with pre-existing neutralizing anti-AGAL antibodies showed a titer increase and one (25.0%) patient a decrease. In patients with anti-AGAL antibodies (n = 4) immune-complex formation was detected.
Conclusion: The pharmacokinetics of pegunigalsidase alfa show different profiles depending on the presence of pre-existing neutralizing antibodies, with reduced plasma half-life and peak enzyme activity after infusion in patients with antibodies. The clinical significance of a reduced pegunigalsidase alfa half-life and the formation of immune complexes in antibody-positive patients needs to be analyzed in future studies.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Funding: Open Access funding enabled and organized by Projekt DEAL. This study received funding from Chiesi GmbH, Germany (investigator initiated non-interventional studies: DJUS21002971, DJUS13008931, DJUS13011311). The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of the article, or the decision to submit it for publication. Conflict of interest: ML received research/travel grants and/or speaker honoraria from Amicus Therapeutics, Sanofi, Chiesi, Sumitomo Pharma, and Takeda. EB received research grants and/or speaker honoraria from Amicus Therapeutics, Sanofi, Chiesi, Takeda, and Eleva. MR received speaker honoraria, congress support, and research grants from Sanofi, Chiesi, and Amicus Therapeutics. MC received speaker honoraria/travel grants from Takeda, Amicus Therapeutics, Idorsia, and Alexion. ERM has nothing to declare. Availability of data and material: The original contributions presented in the study are included in the article and Online Resources; further inquiries can be directed to the corresponding author. Ethics approval: All investigations were performed after approval by the Medical Association of Westphalian-Lippe and the Ethics Committee of the Medical Faculty of the University of Muenster (project no. 2011-347-f, date of report: 7 July 2011) and in accordance with the Declaration of Helsinki. Consent for publication: Written informed consent was obtained from all included patients for analysis and publication. Code availability: Not applicable Authors’ contribution: All authors have contributed to the article by participating in the conception and design (ML), acquisition of data (ML, ERM, MR, MC, EB) or formal analysis (ML, ERM) and interpretation of data (ML, EB), drafting the article (ML, EB) or revising it critically for important intellectual content (ERM, MR, MC). All authors read and approved the final version of the manuscript.
Figures



References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
