

Efficacy of a thermoplastic mask and pneumatic abdominal compression device for immobilization in stereotactic ablative radiotherapy of spine metastases
- PMID: 39616628
- PMCID: PMC11969103
- DOI: 10.1002/acm2.14577
Efficacy of a thermoplastic mask and pneumatic abdominal compression device for immobilization in stereotactic ablative radiotherapy of spine metastases
Abstract
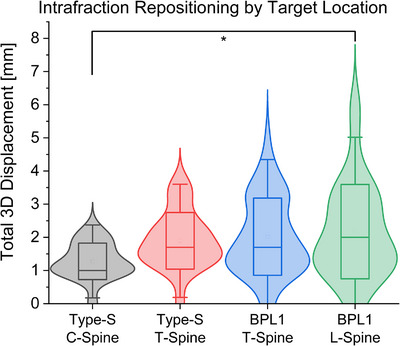
Stereotactic ablative radiotherapy (SABR) has become a key technique in management of spine metastases. With improved control over treatment plan dosimetry, there is a greater need for accurate patient positioning to guarantee agreement between the treatment plan and delivered dose. With serious potential complications such as fracture and myelopathy, the margins of error in SABR of the spine are minimal. In this study, we assessed the performance of two patient immobilization setups in SABR for spinal metastases. First, a Type-S head and shoulders mask (CQ Medical, Avondale, PA), and second, the BPL1 setup, which includes a wing board, vacuum bag, and the Respiratory Belt for the Body Pro-Lok ONE (CQ Medical, Avondale, PA). Immobilization was assessed using image-guided intrafraction repositioning shifts. Required planning target volume (PTV) margins were calculated based on repositioning data for 172 treated fractions using 2 standard deviation (2SD) and analytic approaches. Overall, 91.7% and 74.1% of fractions treated had total 3D repositioning shifts ≤3.0 mm using the Type-S and BPL1 setups, respectively. In the thoracic spine, 43.2% and 46.5% of fractions had shifts ≤1.5 mm for the respective setups. Suggested margins were under 3.5 mm in all directions and use cases. In the posterior-anterior direction, the BPL1 setup had a 0.6 mm smaller suggested margin for the thoracic spine compared to the Type-S setup, at 1.4 mm, calculated using the analytic approach. Both the Type-S and BPL1 setups are effective for immobilization in spine SABR. The Type-S demonstrated superior immobilization in the upper spine and remains the clinical standard for cervical and upper thoracic spine positioning. The BPL1 setup showed effective immobilization in use cases treating the mid-to lower thoracic spine and lumbar spine and remains our clinical standard for those use cases. Results additionally demonstrate feasibility of potential PTV margin reduction.
Keywords: SABR; SBRT; immobilization; motion management; spine metastases; stereotactic ablative radiotherapy; stereotactic body radiation therapy; treatment planning.
© 2024 The Author(s). Journal of Applied Clinical Medical Physics published by Wiley Periodicals LLC on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
YW, DS, CJW, and HTW report active research agreement with CQ Medical (Avondale, PA, USA). YW and DS declare receiving travel funding from CQ Medical.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
