

Lipoprotein (a): Underrecognized Risk with a Promising Future
- PMID: 39618878
- PMCID: PMC11607505
- DOI: 10.31083/j.rcm2511393
Lipoprotein (a): Underrecognized Risk with a Promising Future
Abstract
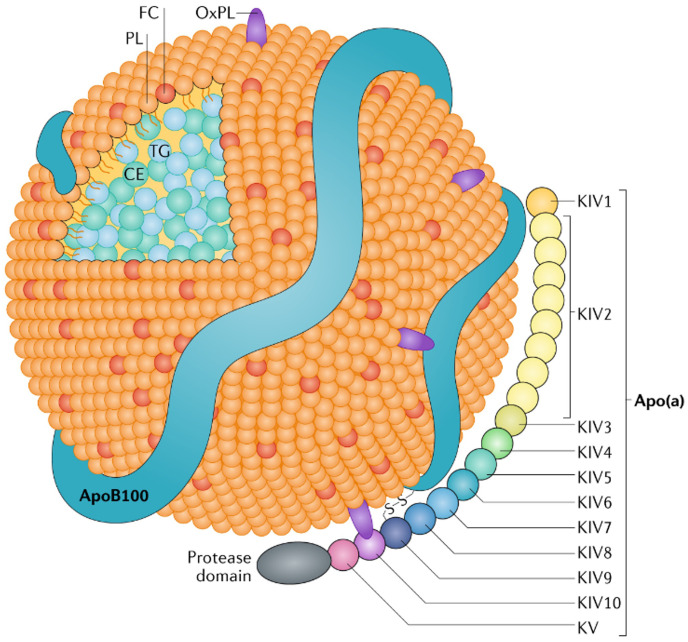
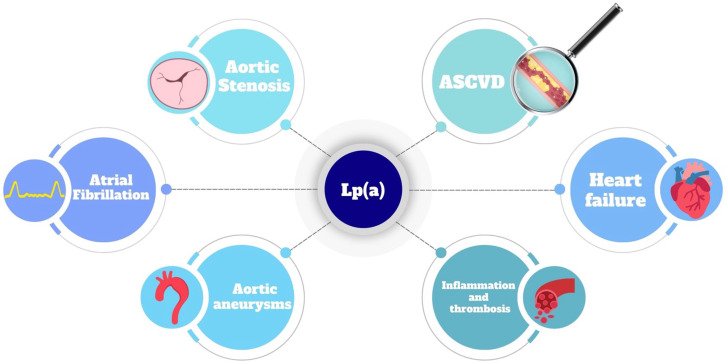
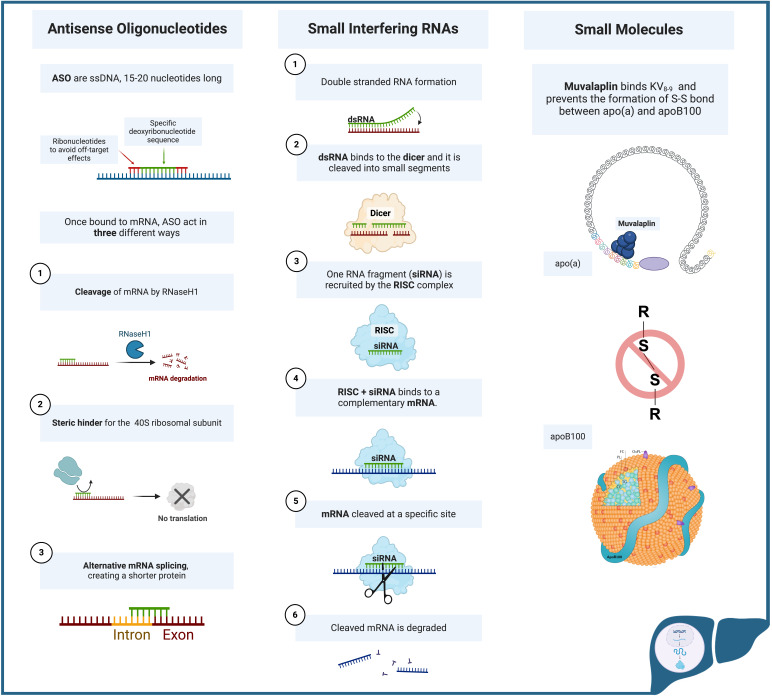
Lipoprotein a (Lp(a)) is a lipid biomarker that binds cholesterol and bears independent cardiovascular risk. Strategies to lower the level of Lp(a) and mitigate such risk are important both for primary and secondary prevention. Currently there are no approved therapies targeting Lp(a) directly. Lipid lowering therapies prescribed routinely may have no effect on Lp(a) levels. Some agents such as niacin and estrogens can significantly decrease Lp(a), but their use is not recommended due to their adverse safety profile. Statins increase Lp(a) levels by 10-20%, questioning the benefit of such therapy when this biomarker is elevated. The Food and Drug Administration (FDA) endorses new agents to address dyslipidemia such as proprotein convertase subtilisin/kexin type 9 inhibitors (PCSK9-i) and Inclisiran, a small interfering RNA. These approaches have been shown to also significantly reduce Lp(a), but more clinical data is needed before implementing their use in clinical practice. Clinical trials are currently ongoing to test the efficacy of newly developed antisense oligonucleotides and small interfering RNAs targeting the gene encoding for Lp(a) in hepatocytes, while other investigations assess small molecules that inhibit Lp(a) assembly. This review summarizes the pathophysiology and clinical implications of Lp(a) elevation, and focuses on proposed Lp(a) therapies and the current state of the clinical trials of such novel agents.
Keywords: ASCVD risk; gene interference therapies; lipoprotein (a).
Copyright: © 2024 The Author(s). Published by IMR Press.
Conflict of interest statement
Matteo Manzato has no conflict of interest; Dr. Vasile has no conflict of interest; Dr. Jaffe presently or in the past has consulted for most of the major in vitro diagnostic companies. He also consults for Moderna and has stock options in RCE Technologies; Dr. Wright reports receiving advisory board fees from Boehringer Ingelheim and past fees for consulting on lipid issues with The Medicines Company.
Figures
References
-
- Wong ND, Fan W, Hu X, Ballantyne C, Hoodgeveen RC, Tsai MY, et al. Lipoprotein(a) and Long-Term Cardiovascular Risk in a Multi-Ethnic Pooled Prospective Cohort. Journal of the American College of Cardiology . 2024;83:1511–1525. - PubMed
-
- Tsimikas S. A Test in Context: Lipoprotein(a): Diagnosis, Prognosis, Controversies, and Emerging Therapies. Journal of the American College of Cardiology . 2017;69:692–711. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
