

Targeting Soluble TGF-β Factors: Advances in Precision Therapy for Pulmonary Arterial Hypertension
- PMID: 39619136
- PMCID: PMC11604486
- DOI: 10.1016/j.jacbts.2024.04.005
Targeting Soluble TGF-β Factors: Advances in Precision Therapy for Pulmonary Arterial Hypertension
Abstract
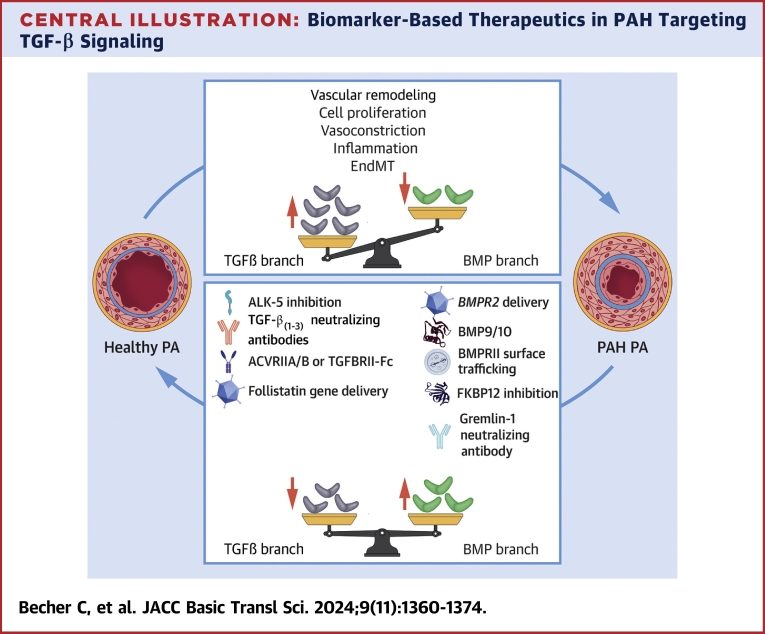
Pulmonary arterial hypertension (PAH) is a rare progressive disease characterized by pulmonary artery vascular remodeling, increased vascular resistance, and subsequent right ventricular hypertrophy and right heart failure. It is triggered by disrupted transforming growth factor (TGF)-β signaling, including loss-of-function mutations in the bone morphogenetic protein (BMP) receptor 2. Emerging treatments aim to inhibit elevated TGF-β levels or enhance diminished endothelial BMP signaling. This review aims to summarize the role of the TGF-β superfamily in the pathobiology of PAH and recent discoveries highlighting altered expression of TGF-β-related soluble factors in PAH patients that can serve as potential biomarkers and drug targets. The discussion focuses on how these altered factors can guide treatment decisions and monitor therapeutic responses, facilitating personalized patient care through the integration of diagnostics and therapy, that is, precision medicine. This approach tailors treatment strategies to individual patients based on their unique disease characteristics.
Keywords: BMPRII; endothelial; miRNAs; small extracellular vesicles; smooth muscle cell.
© 2024 The Authors.
Conflict of interest statement
This work was supported by the Dutch Cardiovascular Alliance (PHAEDRA-IMPACT and DOLPHIN-GENESIS). C. Becher is sponsored by the European Joint Programme on Rare Diseases and The Company of Biologists. Dr Sanchez-Duffhues is sponsored by Fundació la Marato de TV3 (grant 202038), the Spanish Ministerio de Ciencia e Innovación (“Ramon y Cajal” RYC2021-030866-I and PID2022-141212OA-I00 grants). Dr Sanchez-Duffhues and Prof de Man are supported by the BHF-DZHK-DHF 2022/23 award PROMETHEUS. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures



References
-
- Humbert M., Kovacs G., Hoeper M.M., et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022;43:3618–3731. - PubMed
-
- Lau E.M.T., Giannoulatou E., Celermajer D.S., Humbert M. Epidemiology and treatment of pulmonary arterial hypertension. Nat Rev Cardiol. 2017;14:603–614. - PubMed
-
- Benza R.L., Miller D.P., Barst R.J., et al. An evaluation of long-term survival from time of diagnosis in pulmonary arterial hypertension from the REVEAL registry. Chest. 2012;142:448–456. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
