

Update on Prosthesis-Patient Mismatch Following Transcatheter Aortic Valve Replacement in Asian Patients
- PMID: 39619397
- PMCID: PMC11604521
- DOI: 10.1016/j.jacasi.2024.08.010
Update on Prosthesis-Patient Mismatch Following Transcatheter Aortic Valve Replacement in Asian Patients
Abstract
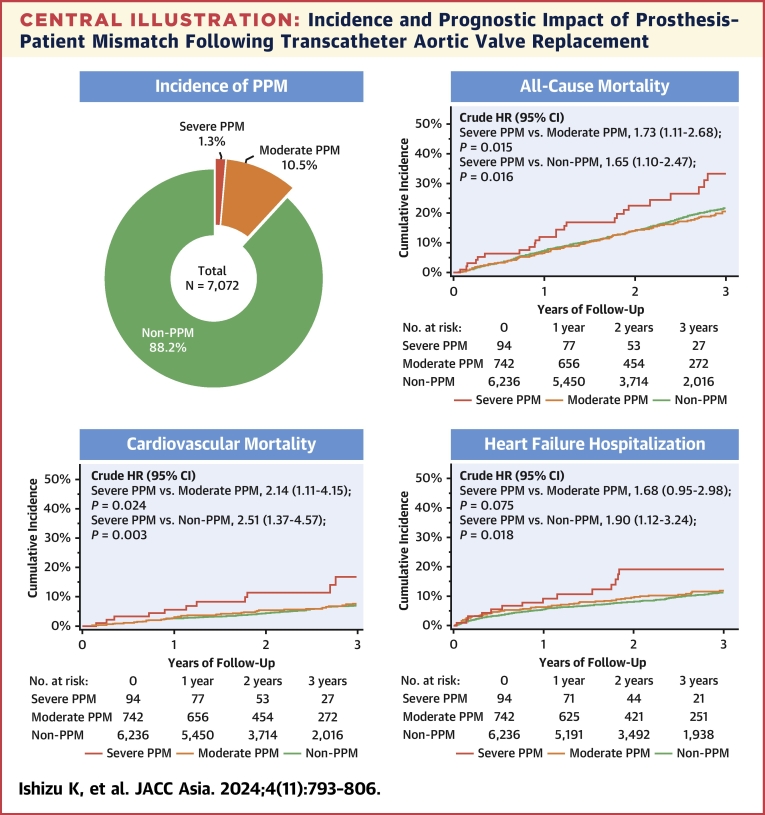
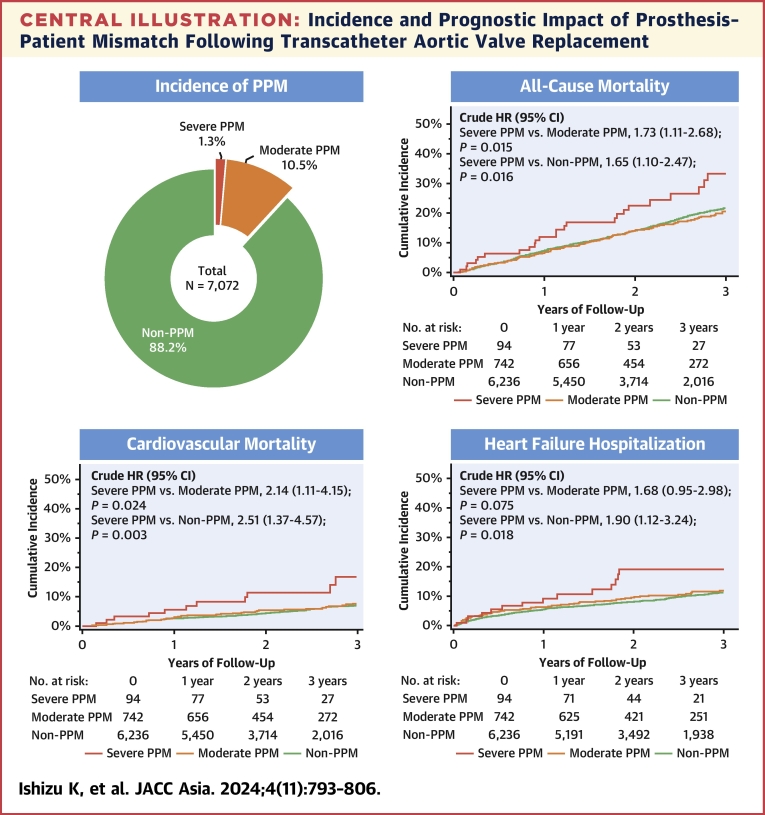
Background: Prosthesis-patient mismatch (PPM) after transcatheter aortic valve replacement (TAVR) is of greater concern in Asians, considering their relatively smaller annular sizes compared with Westerners. However, the prognostic significance of PPM in Asian populations has not been demonstrated.
Objectives: This study aimed to elucidate the prognostic value of PPM after TAVR in Asian patients.
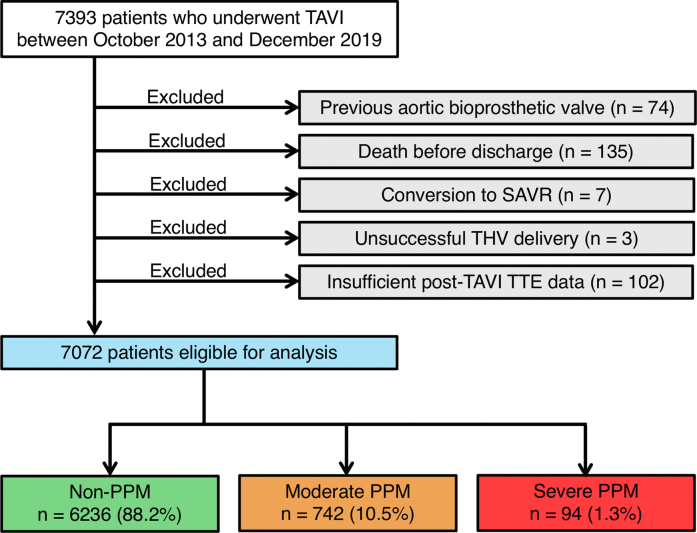
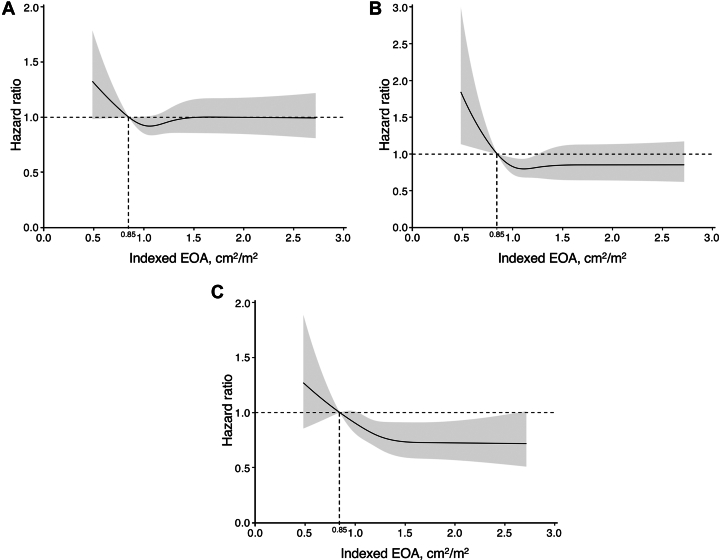
Methods: Patients undergoing TAVR from October 2013 to December 2019 were enrolled from the OCEAN-TAVI (Optimized CathEter vAlvular iNtervention-Transcatheter Aortic Valve Implantation) registry. PPM was classified based on the indexed effective orifice area as severe (≤0.65 cm2/m2) or moderate (0.66-0.85 cm2/m2) in the general population, and severe (≤0.55 cm2/m2) or moderate (0.56-0.70 cm2/m2) in the obese population (body mass index of ≥30 kg/m2).
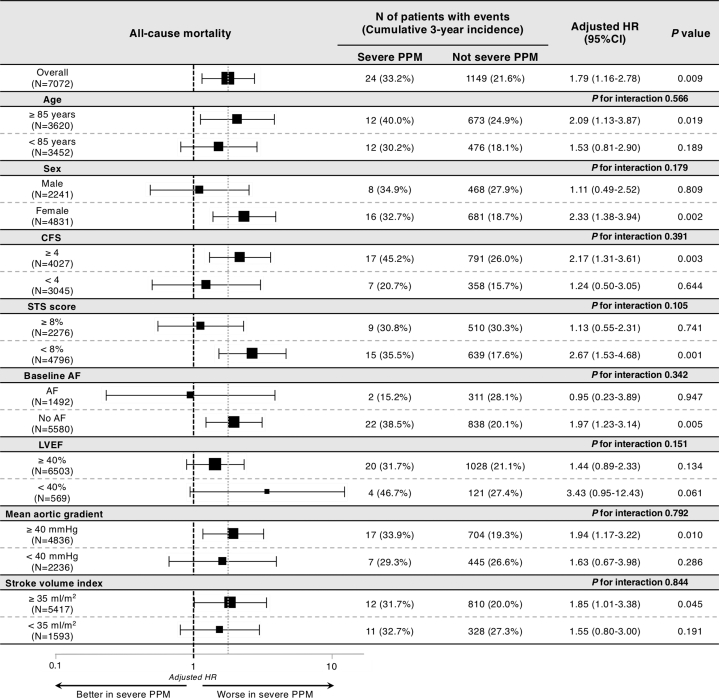
Results: Of the 7,072 eligible patients, moderate and severe PPM were identified in 742 (10.5%) and 94 (1.3%) patients, respectively. Severe PPM relative to non-PPM was independently associated with higher adjusted risks for 3-year all-cause mortality (adjusted HR: 1.79; 95% CI: 1.16-2.78; P = 0.009) and heart failure hospitalization (adjusted HR: 1.88; 95% CI: 1.07-3.28; P = 0.027), whereas no significant difference in these outcomes was observed between moderate PPM and no PPM.
Conclusions: Severe PPM following TAVR was observed in only 1.3% of our Japanese cohort, but was associated with an increased risk of mortality and heart failure hospitalization at 3 years. These results warrant the implementation of preventive strategies to obviate severe PPM after TAVR, also in Asian patients.
Keywords: aortic stenosis; heart failure; long-term outcomes; prosthesis–patient mismatch; transcatheter aortic valve replacement.
© 2024 The Authors.
Conflict of interest statement
The OCEAN-TAVI registry is supported by Edwards Lifesciences, Medtronic, Boston Scientific, Abbott Medical, and Daiichi-Sankyo Company. Dr Izumo is a screening proctor for Edwards Lifesciences. Drs Yohei Ohno, Yashima, and Asami are clinical proctors for Medtronic. Drs Naganuma, Ueno, Mizutani, and Takagi are clinical proctors for Edwards Lifesciences and Medtronic. Drs Masanori Yamamoto, Shirai, Tada, Watanabe, and Hayashida are clinical proctors for Edwards Lifesciences, Abbott Medical, and Medtronic. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Rahimtoola S.H. The problem of valve prosthesis-patient mismatch. Circulation. 1978;58:20–24. - PubMed
-
- Capodanno D., Petronio A.S., Prendergast B., et al. Standardized definitions of structural deterioration and valve failure in assessing long-term durability of transcatheter and surgical aortic bioprosthetic valves: a consensus statement from the European Association of Percutaneous Cardiovascular Interventions (EAPCI) endorsed by the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Eur J Cardiothorac Surg. 2017;52(3):408–417. - PubMed
-
- Clavel M.A., Webb J.G., Pibarot P., et al. Comparison of the hemodynamic performance of percutaneous and surgical bioprostheses for the treatment of severe aortic stenosis. J Am Coll Cardiol. 2009;53(20):1883–1891. - PubMed
-
- Rodes-Cabau J., Pibarot P., Suri R.M., et al. Impact of aortic annulus size on valve hemodynamics and clinical outcomes after transcatheter and surgical aortic valve replacement: insights from the PARTNER Trial. Circ Cardiovasc Interv. 2014;7(5):701–711. - PubMed
LinkOut - more resources
Full Text Sources
