

Creating an 11-year longitudinal substance use harm cohort from linked health and census data to analyse social drivers of health
- PMID: 39620121
- PMCID: PMC11606630
- DOI: 10.23889/ijpds.v9i1.2412
Creating an 11-year longitudinal substance use harm cohort from linked health and census data to analyse social drivers of health
Abstract
Introduction: Research on substance use harm in Canada has been hampered by an absence of linked data to analyse and report on the social drivers of substance use harm.
Objectives: This study aims to address this gap by providing a fully annotated Stata do-file that links sociodemographic data to 11 years of hospitalisation and death outcomes. This do-file will greatly facilitate the creation of provincial and national substance use cohorts using line-level data available through Statistics Canada's Research Data Centres (RDC) program.
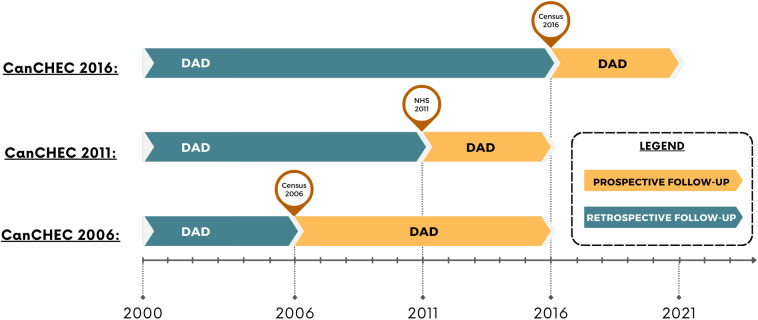
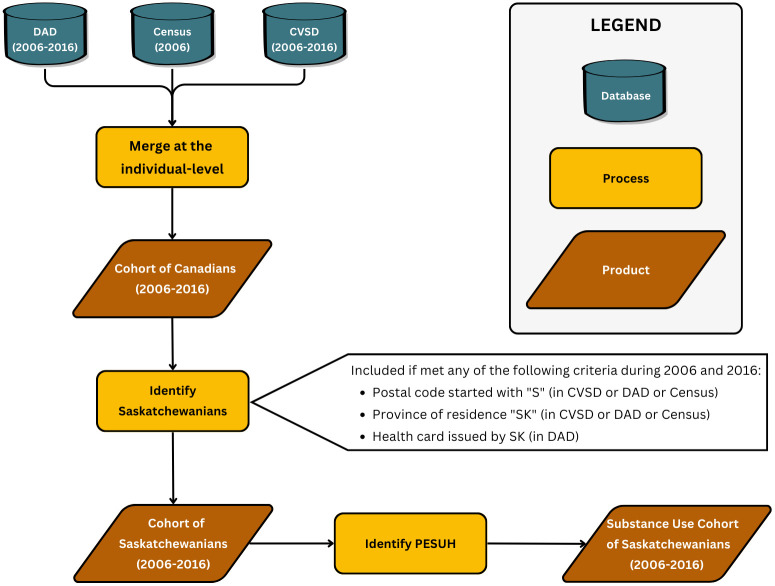
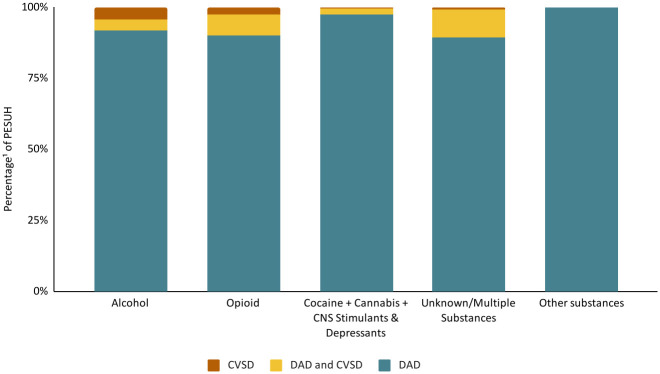
Methods: We used Canadian Census Health and Environment Cohorts (CanCHEC) 2006 to create a cohort of Saskatchewanians followed from 2006 to 2016. We linked sociodemographic information of the 2006 Census (long-form) respondents to their hospitalisation data captured in the Discharge Abstract Database (DAD) (2006 to 2016) and their mortality records in the Canadian Vital Statistics Death Database (CVSD) (2006 to 2016). We developed an algorithm to identify Saskatchewanians who experienced a substance use harm event. We validated the cohort by comparing our descriptive findings with those from other Canadian studies on substance use.
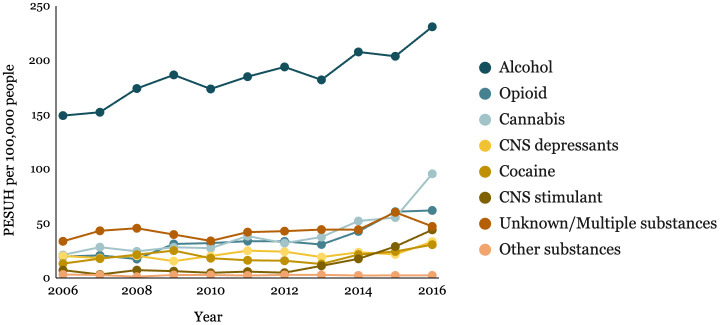
Results: We used CanCHEC, a national data resource, whereas most previous studies have used provincial data resources. Despite this difference in constructing the cohorts, our results showed trends consistent with previous studies, including an overrepresentation of individuals with lower socioeconomic status among the people who experienced substance use harm (PESUH). Similar to other Canadian studies, our results indicate an increasing rate of substance use harm from 2006 to 2016.
Conclusion: This study provides a Stata do-file that compiles a validated substance use cohort using CanCHEC, enabling comprehensive substance use research by linking sociodemographic data with health outcomes. The do-file is likely to save researchers hundreds of hours and accelerate research on the drivers of substance use harms in Canada.
Keywords: censuses; cohort studies; electronic health records; hospital records; longitudinal studies; medical record linkage; mortality; routinely collected health data; social determinants of health; socioeconomic disparities in health; socioeconomic factors; substance-related disorders.
Conflict of interest statement
Statement of conflict of interest: The authors declare that they have no conflict of interest.
Figures
References
-
- Anderson-Baron J, Karekezi K, Koziel J, McCurdy A. Saskatchewan Policy Analysis Case Report: Canadian Harm Reduction Policy Project. Canadian Research Initiative in Substance Misuse; 2017. Available from: https://crismprairies.ca/wp-content/uploads/2018/06/Saskatchewan.pdf
-
- Alsabbagh M, Cooke M, Elliott SJ, Chang F, Shah N-U-H, Ghobrial M, et al.. Stepping up to the Canadian opioid crisis: a longitudinal analysis of the correlation between socioeconomic status and population rates of opioid-related mortality, hospitalization and emergency department visits (2000-2017). Health Promotion & Chronic Disease Prevention in Canada: Research, Policy & Practice 2022;42. 10.24095/hpcdp.42.6.01 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous