

Diuretic efficiency of a single dose of subcutaneous versus oral furosemide after heart failure hospitalization across diuretic resistance strata: A pilot randomized controlled trial
- PMID: 39620306
- PMCID: PMC11860720
- DOI: 10.1002/ejhf.3537
Diuretic efficiency of a single dose of subcutaneous versus oral furosemide after heart failure hospitalization across diuretic resistance strata: A pilot randomized controlled trial
Abstract
Aims: Diuretic resistance (DR) in heart failure (HF) is associated with worse outcomes. Furoscix®, a self-administered subcutaneous (sc) furosemide injection administered via on-body infusor, is approved for HF congestion relief. However, its efficacy in patients with DR post-HF hospitalization remains unknown.
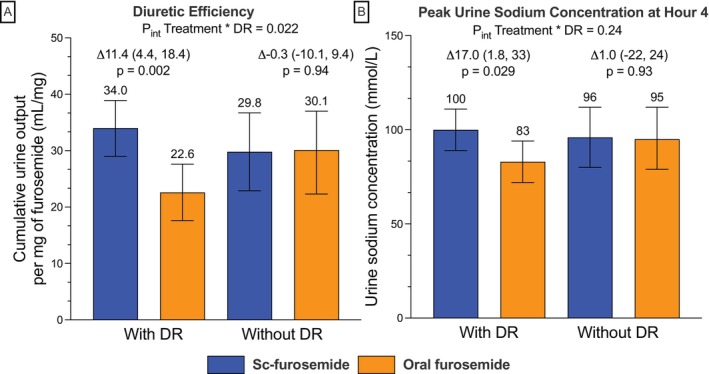
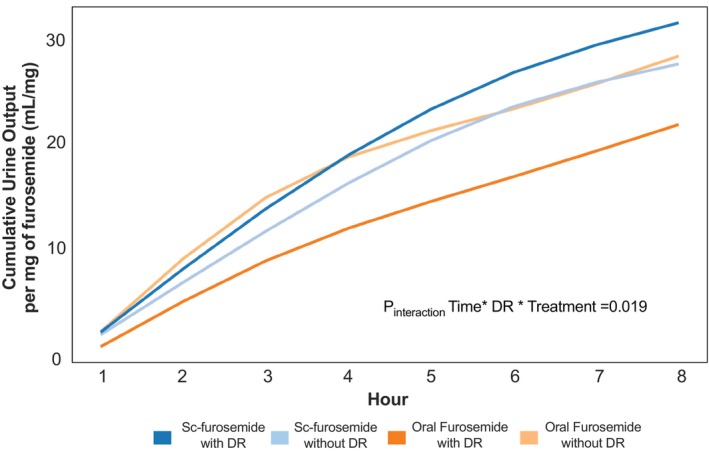
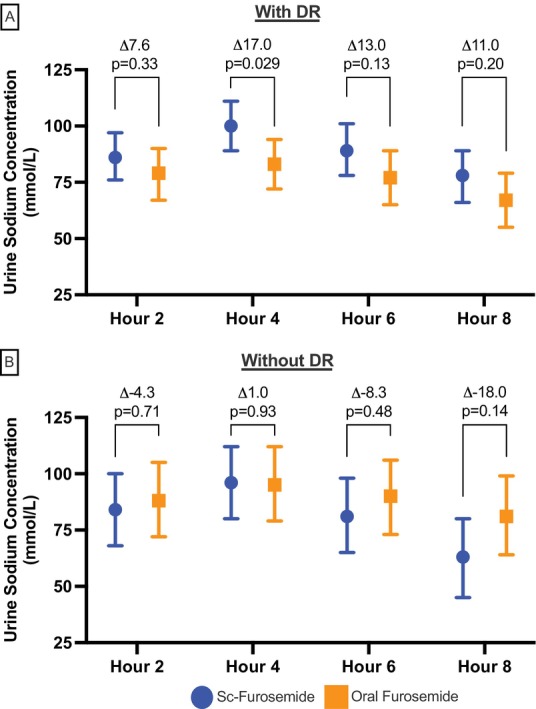
Methods and results: In this open-label pilot randomized controlled trial, 70 participants were randomized within 14 days post-HF hospitalization to receive a single dose of 80 mg sc furosemide or home oral dose furosemide. Enrolment was stratified by presence of DR (admission BAN-ADHF score ≥12) with a 2:1 enrolment of those with versus without DR. Key outcomes included diuretic efficiency, the total urine output per mg of diuretic administered, and peak urine sodium within 8 h of dose administration. Treatment effects were calculated as the difference in estimated marginal means across study groups and DR strata using linear mixed-effect models. Overall, 70 participants were enrolled (57 years, 27% female, 70% Black, 79% with HF with reduced ejection fraction). Participants with DR (n = 46) had worse kidney function, higher N-terminal pro-B-type natriuretic peptide, and higher home diuretic dose. Among participants with DR, sc furosemide versus oral furosemide led to significantly greater diuretic efficiency (34.0 vs. 22.6 ml/mg, p = 0.002) and peak urine sodium (100 vs. 83 mmol/L, p = 0.029), while participants without DR had similar diuretic efficiency (29.8 vs. 30.1 ml/mg, p = 0.94) and peak urine sodium (96 vs. 95 mmol/L, p = 0.93) across both treatments. DR significantly modified the effect of sc versus oral furosemide on diuretic efficiency (pinteraction: treatment × diuretic resistance = 0.022).
Conclusion: Single-dose sc furosemide was associated with greater diuretic efficiency and peak urine sodium than oral furosemide in participants with DR discharged following recent HF hospitalization.
Keywords: Diuretic resistance; Heart failure; Subcutaneous furosemide.
© 2024 The Author(s). European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures
Similar articles
-
Efficacy of Intravenous Furosemide Versus a Novel, pH-Neutral Furosemide Formulation Administered Subcutaneously in Outpatients With Worsening Heart Failure.JACC Heart Fail. 2018 Jan;6(1):65-70. doi: 10.1016/j.jchf.2017.10.001. Epub 2017 Dec 6. JACC Heart Fail. 2018. PMID: 29226816 Free PMC article. Clinical Trial.
-
Avoiding Treatment in Hospital With Subcutaneous Furosemide for Worsening Heart Failure: A Pilot Study (AT HOME-HF).JACC Heart Fail. 2024 Nov;12(11):1830-1841. doi: 10.1016/j.jchf.2024.07.015. Epub 2024 Sep 11. JACC Heart Fail. 2024. PMID: 39269392 Clinical Trial.
-
Dose of furosemide before admission predicts diuretic efficiency and long-term prognosis in acute heart failure.ESC Heart Fail. 2022 Feb;9(1):656-666. doi: 10.1002/ehf2.13696. Epub 2021 Nov 11. ESC Heart Fail. 2022. PMID: 34766460 Free PMC article.
-
The Role of Subcutaneous Furosemide in Heart Failure Management: A Systematic Review.Curr Cardiol Rep. 2024 Nov;26(11):1285-1296. doi: 10.1007/s11886-024-02124-4. Epub 2024 Oct 1. Curr Cardiol Rep. 2024. PMID: 39352583 Free PMC article.
-
Basal natriuresis as a predictor of diuretic resistance and clinical evolution in acute heart failure.Curr Probl Cardiol. 2024 Aug;49(8):102674. doi: 10.1016/j.cpcardiol.2024.102674. Epub 2024 May 23. Curr Probl Cardiol. 2024. PMID: 38795800 Review.
References
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA Guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2022;79:e263–e421. 10.1016/j.jacc.2021.12.012 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
