

Home-Based Exercise and Self-Management After Lung Cancer Resection: A Randomized Clinical Trial
- PMID: 39621348
- PMCID: PMC11612835
- DOI: 10.1001/jamanetworkopen.2024.47325
Home-Based Exercise and Self-Management After Lung Cancer Resection: A Randomized Clinical Trial
Abstract
Importance: Patients with lung cancer have poor physical functioning and quality of life. Despite promising outcomes for those who undertake exercise programs, implementation into practice of previously tested hospital-based programs is rare.
Objective: To evaluate a home-based exercise and self-management program for patients after lung resection.
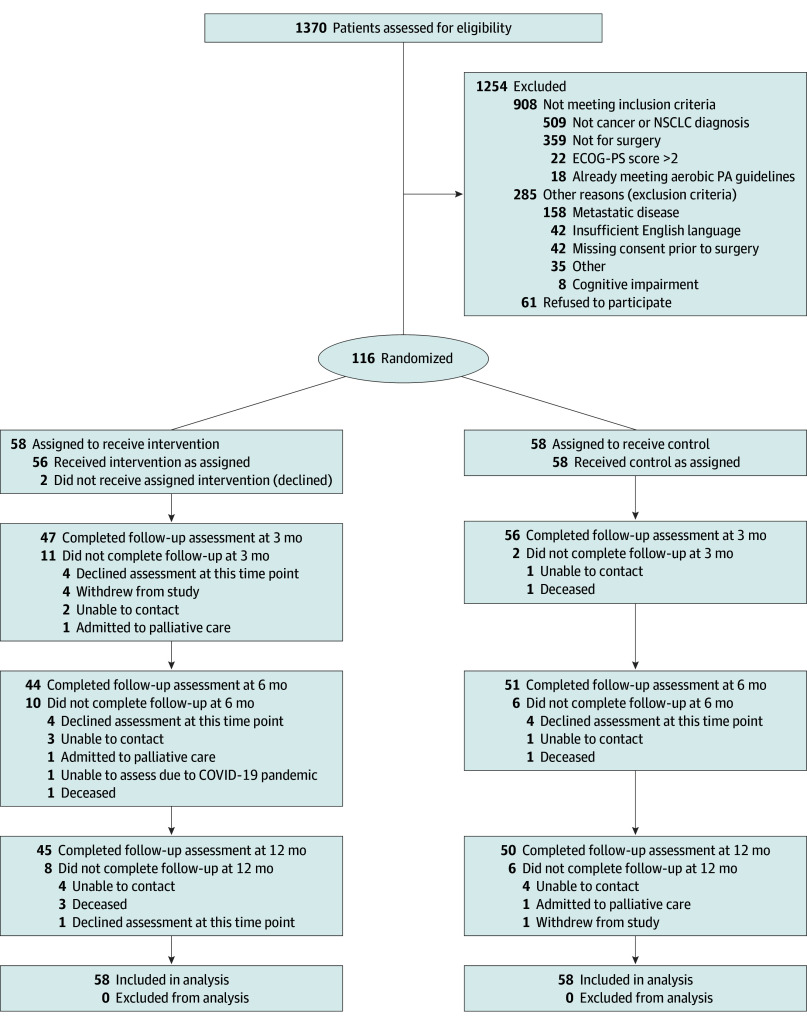
Design, setting, and participants: A randomized clinical trial with assessor blinding was conducted among 116 patients undergoing surgery for non-small cell lung cancer from November 23, 2017, to July 31, 2023, at tertiary hospitals in Australia. Patients were followed up for 12 months postoperatively.
Intervention: Patients randomized to the intervention group received a postoperative 3-month home-based exercise and self-management program, supported by weekly physiotherapist-led telephone consultations. Patients randomized to the control group received usual care.
Main outcomes and measures: The primary outcome was self-reported physical function (30-item European Organization for the Research and Treatment of Cancer Core Quality of Life Questionnaire [EORTC QLQ-C30] score) at 3 months. Secondary outcomes included objective measures of physical function and exercise capacity (at 3 and 6 months) and patient-reported outcomes including quality of life (at 3 and 6 months, with some questionnaires completed at 12 months). Analysis was performed on an intent-to-treat basis.
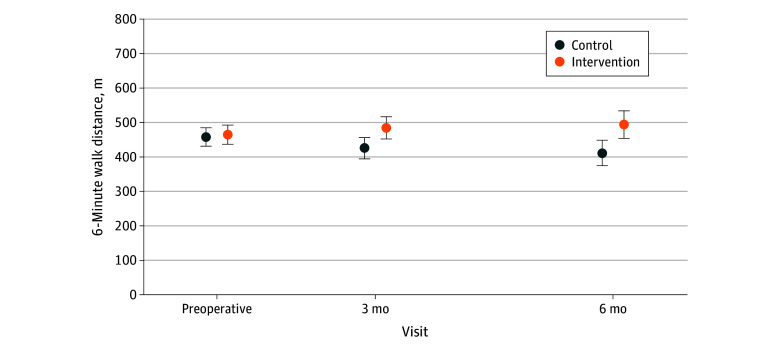
Results: A total of 1370 patients were screened, with 177 eligible and 116 consented (mean [SD] age, 66.4 [9.6] years; 68 women [58.6%]). Of these 116 patients, 58 were randomized to the intervention and 58 to the control. A total of 103 patients (88.8%) completed assessments at 3 months, 95 (81.9%) at 6 months, and 95 (81.9%) at 12 months. There were no statistically significant differences between the intervention and control groups for self-reported physical function (EORTC QLQ-C30 physical functioning domain score) at the 3-month primary end point (mean [SD] score, 77.3 [20.9] vs 76.3 [18.8]; mean difference, 1.0 point [95% CI, -6.0 to 8.0 points]). Patients in the intervention group, compared with the control group, had significantly greater exercise capacity (6-minute walk distance: mean difference, 39.7 m [95% CI, 6.8-72.6 m]), global quality of life (mean difference, 7.1 points [95% CI, 0.4-13.8 points]), and exercise self-efficacy (mean difference, 16.0 points [95% CI, 7.0-24.9 points]) at 3 months as well as greater objectively measured physical function (Short Physical Performance Battery score: mean difference, 0.8 points [95% CI, 0.1-1.6 points]), exercise capacity (6-minute walk distance: mean difference, 50.9 m [95% CI, 6.7-95.1 m]), and exercise self-efficacy (mean difference, 10.1 points [95% CI, 1.9-18.2 points]) at 6 months. One minor adverse event and no serious adverse events occurred.
Conclusions and relevance: In this randomized clinical trial, a postoperative home-based exercise and self-management program did not improve self-reported physical function in patients with lung cancer. However, it did improve other important clinical outcomes. Implementation of this program into lung cancer care should be considered.
Trial registration: http://anzctr.org.au Identifier: ACTRN12617001283369.
Conflict of interest statement
Figures
Comment in
- doi: 10.1001/jamanetworkopen.2024.47287
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
