

A latent class assessment of healthcare access factors and disparities in breast cancer care timeliness
- PMID: 39621782
- PMCID: PMC11649116
- DOI: 10.1371/journal.pmed.1004500
A latent class assessment of healthcare access factors and disparities in breast cancer care timeliness
Abstract
Background: Delays in breast cancer diagnosis and treatment lead to worse survival and quality of life. Racial disparities in care timeliness have been reported, but few studies have examined access at multiple points along the care continuum (diagnosis, treatment initiation, treatment duration, and genomic testing).
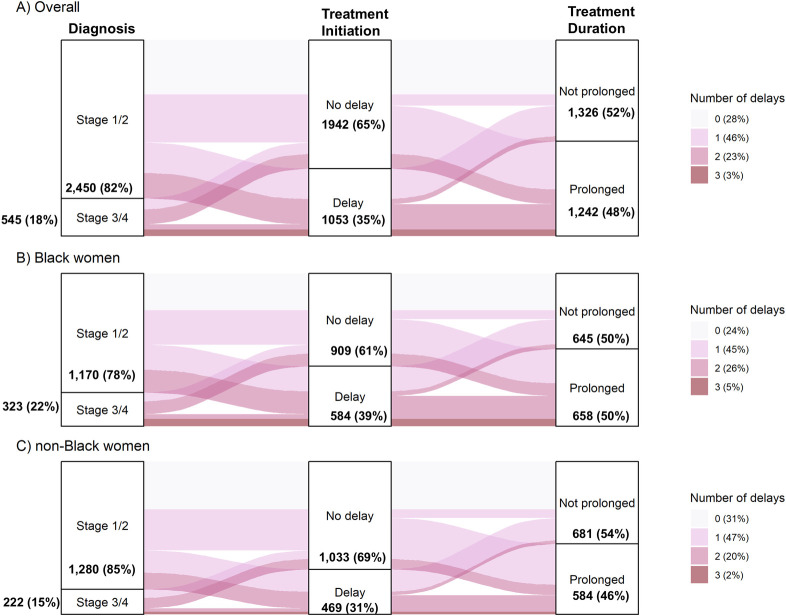
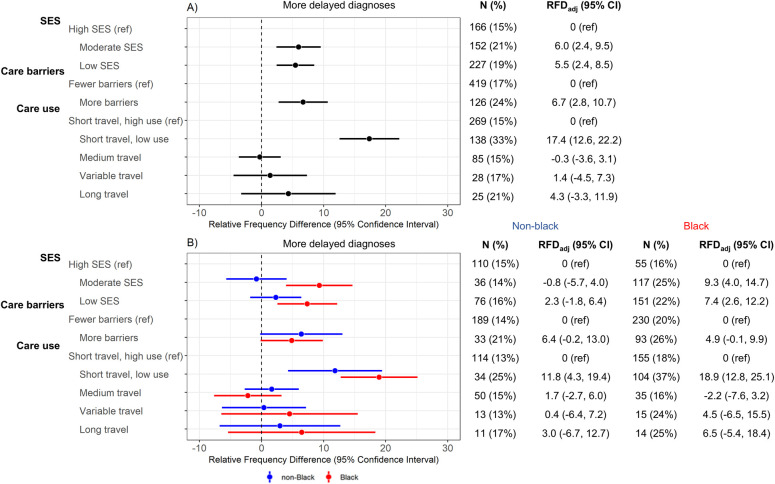
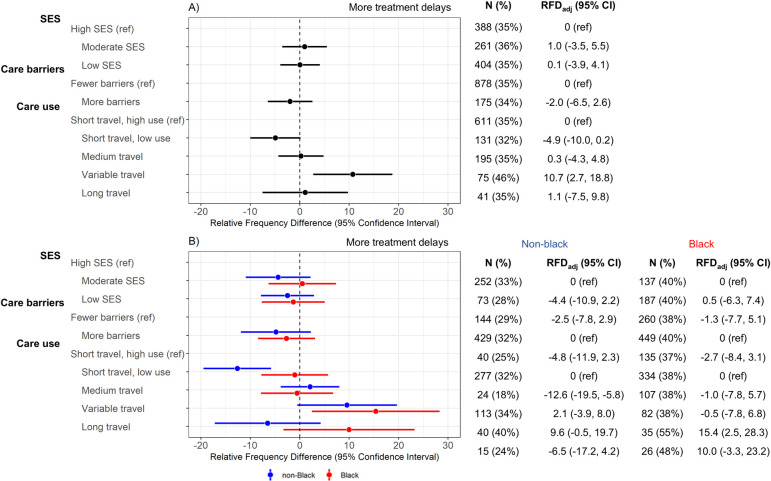
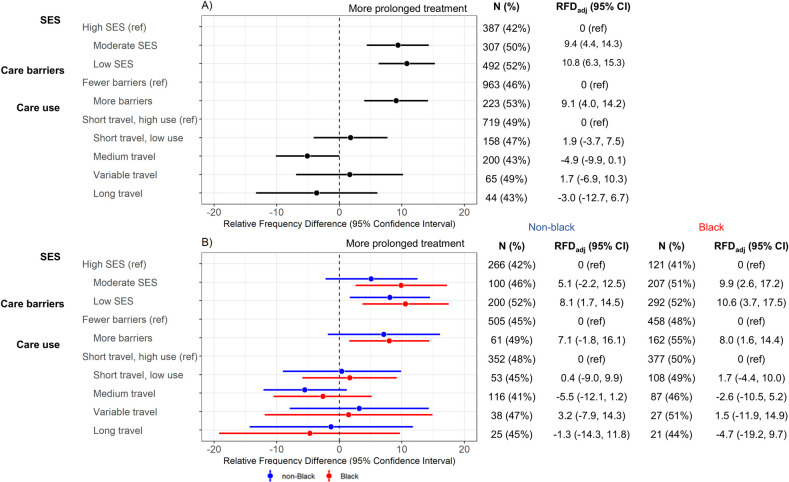
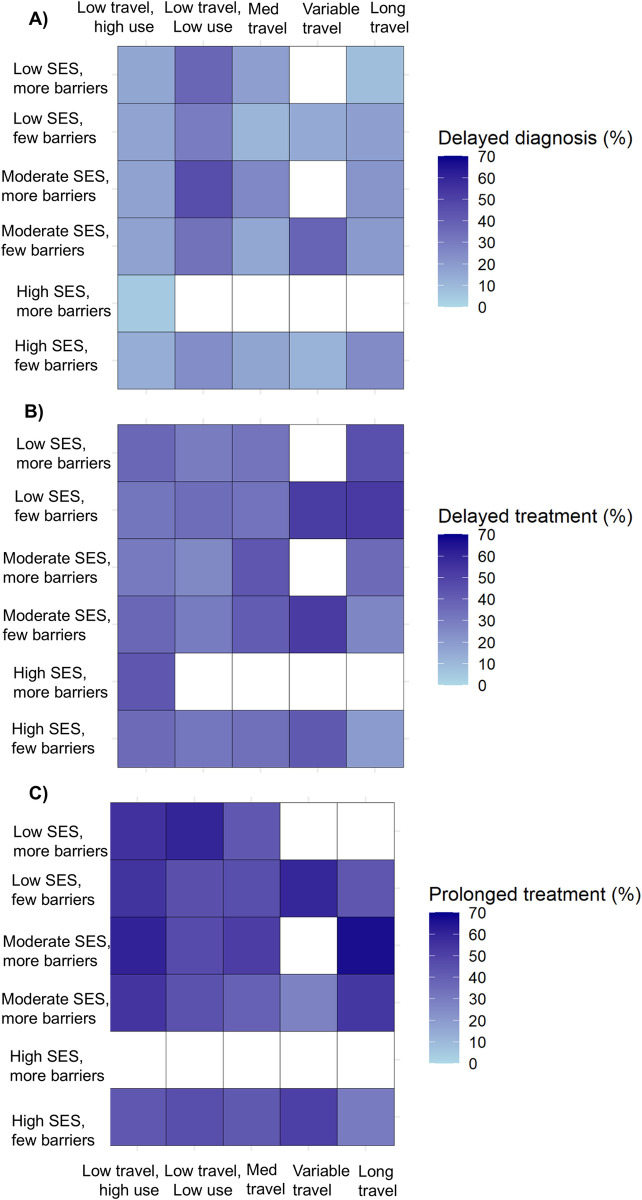
Methods and findings: The Carolina Breast Cancer Study (CBCS) Phase 3 is a population-based, case-only cohort (n = 2,998, 50% black) of patients with invasive breast cancer diagnoses (2008 to 2013). We used latent class analysis (LCA) to group participants based on patterns of factors within 3 separate domains: socioeconomic status ("SES"), "care barriers," and "care use." These classes were evaluated in association with delayed diagnosis (approximated with stages III-IV at diagnosis), delayed treatment initiation (more than 30 days between diagnosis and first treatment), prolonged treatment duration (time between first and last treatment-by treatment modality), and receipt of OncotypeDx genomic testing (evaluated among patients with early stage, ER+ (estrogen receptor-positive), HER2- (human epidermal growth factor receptor 2-negative) disease). Associations were evaluated using adjusted linear-risk regression to estimate relative frequency differences (RFDs) with 95% confidence intervals (CIs). Delayed diagnosis models were adjusted for age; delayed and prolonged treatment models were adjusted for age and tumor size, stage, and grade at diagnosis; and OncotypeDx models were adjusted for age and tumor size and grade. Overall, 18% of CBCS participants had late stage/delayed diagnosis, 35% had delayed treatment initiation, 48% had prolonged treatment duration, and 62% were not OncotypeDx tested. Black women had higher prevalence for each outcome. We identified 3 latent classes for SES ("high SES," "moderate SES," and "low SES"), 2 classes for care barriers ("few barriers," "more barriers"), and 5 classes for care use ("short travel/high preventive care," "short travel/low preventive care," "medium travel," "variable travel," and "long travel") in which travel is defined by estimated road driving time. Low SES and more barriers to care were associated with greater frequency of delayed diagnosis (RFDadj = 5.5%, 95% CI [2.4, 8.5]; RFDadj = 6.7%, 95% CI [2.8,10.7], respectively) and prolonged treatment (RFDadj = 9.7%, 95% CI [4.8 to 14.6]; RFDadj = 7.3%, 95% CI [2.4 to 12.2], respectively). Variable travel (short travel to diagnosis but long travel to surgery) was associated with delayed treatment in the entire study population (RFDadj = 10.7%, 95% CI [2.7 to 18.8]) compared to the short travel, high use referent group. Long travel to both diagnosis and surgery was associated with delayed treatment only among black women. The main limitations of this work were inability to make inferences about causal effects of individual variables that formed the latent classes, reliance on self-reported socioeconomic and healthcare history information, and generalizability outside of North Carolina, United States of America.
Conclusions: Black patients face more frequent delays throughout the care continuum, likely stemming from different types of access barriers at key junctures. Improving breast cancer care access will require intervention on multiple aspects of SES and healthcare access.
Copyright: © 2024 Dunn et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
M.L.R. received consulting fees from Concert Genetics and National Committee for Quality Assurance, unrelated to the submitted work.
Figures
References
-
- National Cancer Institute. Stage at Diagnosis: Cancer Trends Progress Report. [cited 2024. Mar 15]. Available from: https://progressreport.cancer.gov/diagnosis/stage.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
