

Adverse cardiovascular events and cardiac imaging findings in patients on immune checkpoint inhibitors
- PMID: 39621799
- PMCID: PMC11611253
- DOI: 10.1371/journal.pone.0314555
Adverse cardiovascular events and cardiac imaging findings in patients on immune checkpoint inhibitors
Abstract
Background: There is an urgent need to better understand the diverse presentations, risk factors, and outcomes of immune checkpoint inhibitor (ICI)-associated cardiovascular toxicity. There remains a lack of consensus surrounding cardiovascular screening, risk stratification, and clinical decision-making in patients receiving ICIs.
Methods: We conducted a single center retrospective cohort study including 2165 cancer patients treated with ICIs between 2013 and 2020. The primary outcome was adverse cardiovascular events (ACE): a composite of myocardial infarction, coronary artery disease, stroke, peripheral vascular disease, arrhythmias, heart failure, valvular disease, pericardial disease, and myocarditis. Secondary outcomes included all-cause mortality and the individual components of ACE. We additionally conducted an imaging substudy examining imaging characteristics from echocardiography (echo) and cardiac magnetic resonance (CMR) imaging.
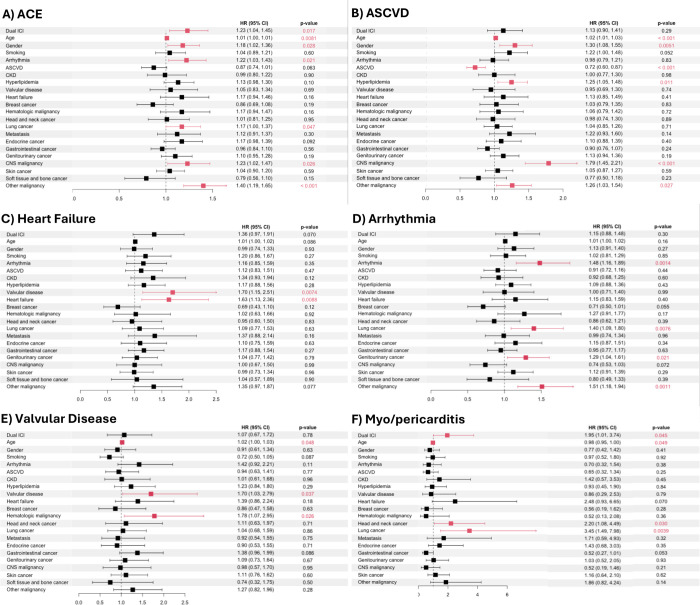
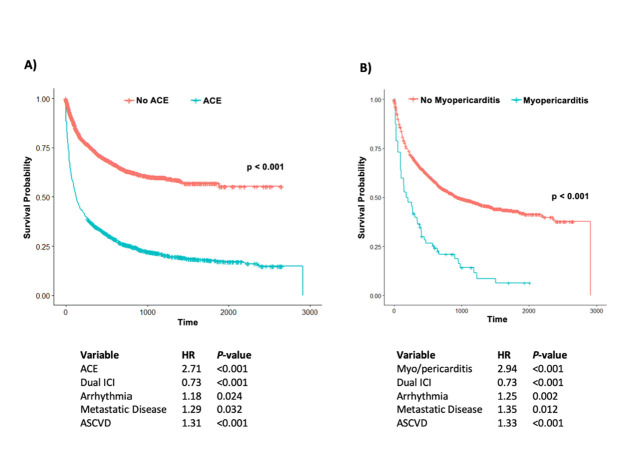
Results: In our cohort, 44% (n = 962/2165) of patients experienced ACE. In a multivariable analysis, dual ICI therapy (hazard ratio [HR] 1.23, confidence interval [CI] 1.04-1.45), age (HR 1.01, CI 1.00-1.01), male sex (HR 1.18, CI 1.02-1.36), prior arrhythmia (HR 1.22, CI 1.03-1.43), lung cancer (HR 1.17, CI 1.01-1.37), and central nervous system (CNS) malignancy (HR 1.23, CI 1.02-1.47), were independently associated with increased ACE. ACE was independently associated with a 2.7-fold increased risk of mortality (P<0.001). Dual ICI therapy was also associated with a 2.0-fold increased risk of myo/pericarditis (P = 0.045), with myo/pericarditis being associated with a 2.9-fold increased risk of mortality (P<0.001). However, the cardiovascular risks of dual ICI therapy were offset by its mortality benefit, with dual ICI therapy being associated with a ~25% or 1.3-fold decrease in mortality. Of those with echo prior to ICI initiation, 26% (n = 115/442) had abnormal left ventricular ejection fraction or global longitudinal strain, and of those with echo after ICI initiation, 28% (n = 207/740) had abnormalities. Of those who had CMR imaging prior to ICI initiation, 43% (n = 9/21) already had left ventricular dysfunction, 50% (n = 10/20) had right ventricular dysfunction, 32% (n = 6/19) had left ventricular late gadolinium enhancement, and 9% (n = 1/11) had abnormal T2 imaging.
Conclusion: Dual ICI therapy, prior arrhythmia, older age, lung and CNS malignancies were independently associated with an increased risk of ACE, and dual ICI therapy was also independently associated with an increased risk of myo/pericarditis, highlighting the utmost importance of cardiovascular risk factor optimization in this particularly high-risk population. Fortunately, the occurrence of myo/pericarditis was relatively uncommon, and the overall cardiovascular risks of dual ICI therapy appeared to be offset by a significant mortality benefit. The use of multimodal cardiac imaging can be helpful in stratifying risk and guiding preventative cardiovascular management in patients receiving ICIs.
Copyright: © 2024 Kwan et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
