

Population-Based Study of the Epidemiology of Stiff Person Syndrome in a Large Colorado-Based Health System
- PMID: 39621949
- PMCID: PMC11606148
- DOI: 10.1212/WNL.0000000000210078
Population-Based Study of the Epidemiology of Stiff Person Syndrome in a Large Colorado-Based Health System
Abstract
Background and objectives: Stiff person syndrome spectrum disorder (SPSD) is a rare autoimmune disorder characterized by progressive muscle stiffness and painful spasms with an estimated prevalence of 1-2 cases per million people. Population-based epidemiologic studies are lacking because of both poor patient capture and the lack of standardized diagnostic criteria. Objectives of this study were to describe the incidence and prevalence of SPSD within the University of Colorado Health (UCH) system and apply previously proposed published criteria for SPSD within this population.
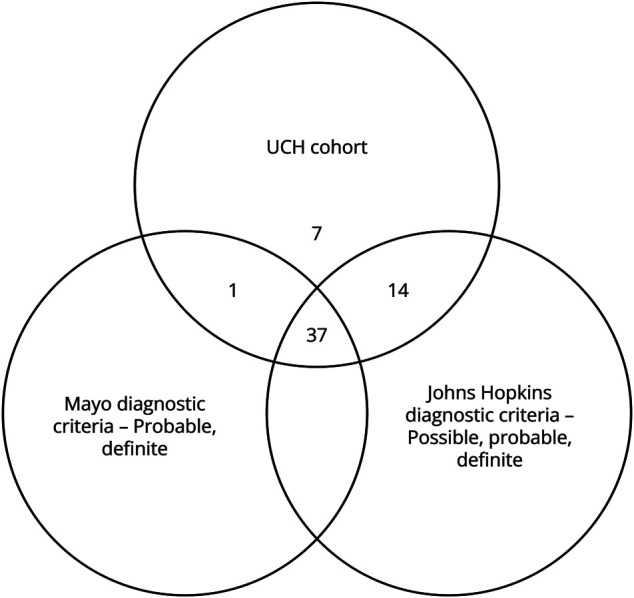
Methods: We queried Health Data Compass, an electronic health data repository for a large academic health care system, from 2012 through 2022 for all patients older than 18 years with International Classification of Diseases, 10th Revision (ICD-10) codes pertaining to stiff person syndrome. Records were reviewed for diagnostic confirmation. We calculated yearly and period prevalence and incidence rates based on observable person-time exposure of our cohort. We applied previously published Mayo Clinic and Johns Hopkins criteria for SPSD and compared period prevalence based on each criterion and evaluated for agreement.
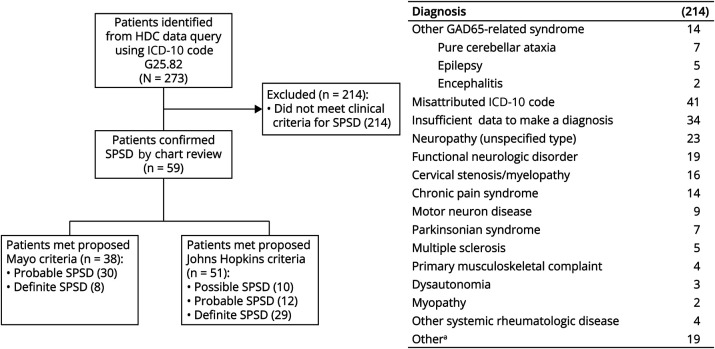
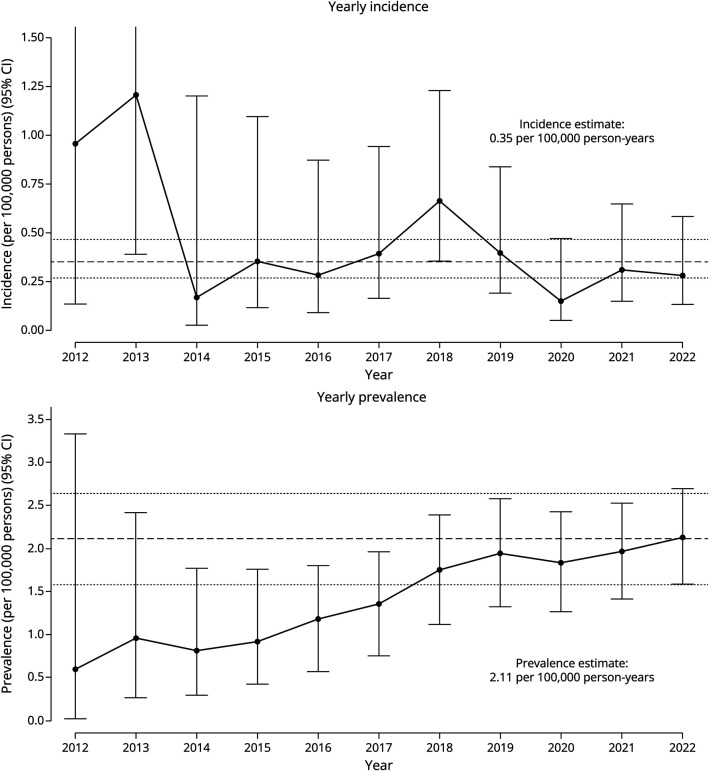
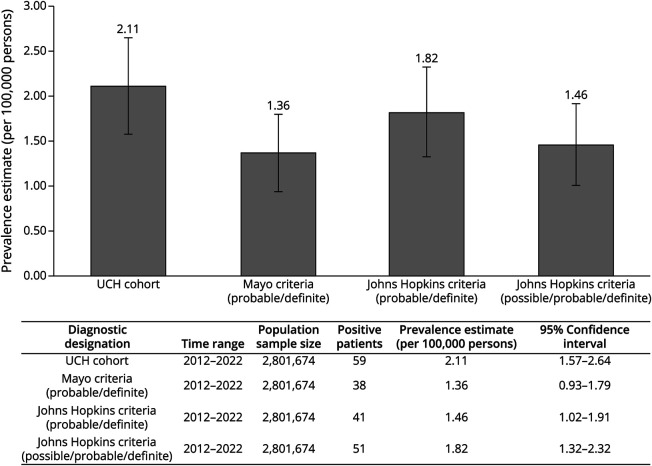
Results: Two hundred and seventy-three patients met the initial inclusion criteria using ICD-10 codes; 59 were confirmed to have SPSD. The mean age was 49.7 years (SD = 12.9), 59.3% were female, 59.3% were considered antibody positive. The total database population over the interval was 2,801,674 persons. The estimated prevalence of SPSD based on our UCH cohort was 2.11 (95% CI 1.57-2.64) per 100,000 persons. The average yearly incidence was 0.35 per 100,000 person-years (95% CI 0.27-0.46). Applying different clinical diagnostic criteria, the estimated prevalence ranged from 1.36 (95% CI 0.93-1.79) to 1.82 (95% CI 1.32-2.32) per 100,000 persons.
Discussion: We describe a prevalence of SPSD of 2.11 per 100,000 persons in our UCH cohort. Prevalence estimates differed depending on which clinical diagnostic criteria were applied and whether possible SPSD cases were included. Using the most stringent criteria for diagnosis, we report a prevalence of 1.36 per 100,000 persons. While our study uniquely captures many US demographic groups, limitations remain because this is a retrospective review of a single system. Additional studies are needed to determine whether these results are representative of a national or global population.
Conflict of interest statement
P.D. Crane, S. Sillau, R. Dreher, R. Fix, P. Winters, R.V. Coevering, E. Engebretson, B. Valdez, and E.A. Matthews report no disclosures. K.V. Nair reports research grants from Genentech, PhRMA Foundation, Bristol Myers Squibb, Alexion, Squibb, Novartis, Horizon Biogen, and National Institute of Neurological Disorders and Stroke, and consulting fees from Bristol Myers Squibb, Novartis, Biogen, TG Therapeutics, Genentech and EMD Serono. In addition, she reports speakers bureau affiliation with Sanofi-Genzyme, Amgen and AJCM speaker series. A.M. Carlson reports unrelated grant funding from Horizon Therapeutics and recent service on the Health Services Subcommittee for the American Academy of Neurology. A.L. Piquet reports research grants from the University of Colorado, research funding from the Endowed Chair supported by the Céline Dion Foundation, Rocky Mountain MS Center, and the Foundation for Sarcoidosis; consulting fees from Genentech/Roche, UCB, EMD Serono, Kyverna and Alexion; honoraria from MedLink; and publication royalties from Springer as co-editor of a medical textbook. Go to
Figures
References
-
- Moersch FP, Woltman HW. Progressive fluctuating muscular rigidity and spasm (“stiff-man” syndrome); report of a case and some observations in 13 other cases. Proc Staff Meet Mayo Clin. 1956;31(15):421-427. - PubMed
-
- Barker RA, Revesz T, Thom M, Marsden CD, Brown P. Review of 23 patients affected by the stiff man syndrome: clinical subdivision into stiff trunk (man) syndrome, stiff limb syndrome, and progressive encephalomyelitis with rigidity. J Neurol Neurosurg Psychiatry. 1998;65(5):633-640. doi: 10.1136/jnnp.65.5.633. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous