

Exemplar Hospital Initiation Trial to Enhance Treatment Engagement (EXHIT ENTRE): protocol for CTN-0098 an open-label randomized comparative effectiveness trial of extended-release buprenorphine versus treatment as usual on post-hospital treatment engagement for hospitalized patients with opioid use disorder
- PMID: 39623502
- PMCID: PMC11610182
- DOI: 10.1186/s13722-024-00510-5
Exemplar Hospital Initiation Trial to Enhance Treatment Engagement (EXHIT ENTRE): protocol for CTN-0098 an open-label randomized comparative effectiveness trial of extended-release buprenorphine versus treatment as usual on post-hospital treatment engagement for hospitalized patients with opioid use disorder
Abstract
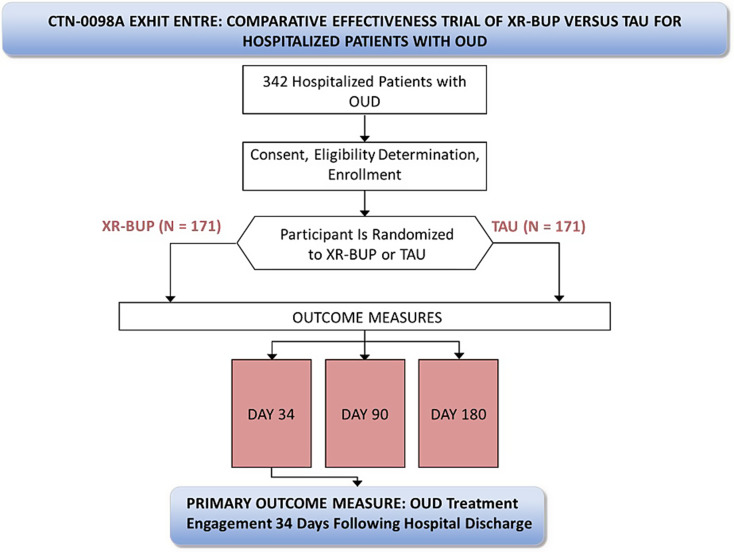
Background: Hospitalizations involving opioid use disorder (OUD) are increasing. Addiction consultation services (ACS) initiate medications for opioid use disorder (MOUD) in hospital settings and arrange post-hospital follow-up for ongoing MOUD care. Engagement in MOUD following hospital discharge is hampered by challenges in timely access to MOUD. This protocol describes an open-label randomized comparative effectiveness trial comparing ACS treatment as usual (TAU) to a single injection of a 28-day formulation extended-release buprenorphine (XR-BUP) on MOUD engagement 34-days following hospital discharge.
Methods: Six U.S. hospitals with ACS capable of prescribing all MOUD (i.e., methadone, buprenorphine, and extended-release naltrexone) recruit and randomize hospitalized patients with OUD who have not been on MOUD in the fourteen days prior to hospitalization. TAU may consist of any MOUD other than XR-BUP. Participants randomized to XR-BUP may receive any MOUD throughout their hospital stay and receive a 28-day XR-BUP injection within 72-hours of anticipated hospital discharge. There is no intervention beyond hospital stay. Participants are followed 34-, 90-, and 180-days following hospital discharge. The primary outcome is engagement in any MOUD 34-days following hospital discharge, which we hypothesize will be greater in the XR-BUP group. Randomizing 342 participants (171 per arm) provides 90% power to detect difference in the primary outcome between groups with an odds ratio of 2.1. Safety, secondary, and exploratory outcomes include: adverse events, MOUD engagement on days 90 and 180, opioid positive urine drug tests, self-reported drug use, hospital readmissions and emergency department visits, use of non-opioid drugs, fatal and non-fatal opioid overdose, all-cause mortality, quality of life, and cost-effectiveness. Data are analyzed by intention-to-treat, with pre-planned per-protocol and other secondary analyses that examine gender as an effect modifier, differences between groups, and impact of missingness.
Discussion: Engagement in MOUD care following hospitalization in individuals with OUD is low. This randomized comparative effectiveness trial can inform hospital ACS in medication selection to improve MOUD engagement 34-days following hospital discharge.
Trial registration: NCT04345718.
Keywords: Comparative effectiveness; Hospital; Medications for opioid use disorder; Opioid use disorder; Protocol.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol was approved by Advarra (Protocol number Pro00047336), a commercial Institutional Review Board. Competing interests: The authors declare no competing interests.
References
-
- Bedi P, Rai MP, Bumrah K, Singh VK, Arora TK, Singh T. Pattern and burden of opioid-related hospitalizations in the USA from 2016 to 2018. Br J Clin Pharmacol. 2021;87(11):4366–74. 10.1111/bcp.14857. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
