

Fecal deoxycholic acid associates with diet, intestinal microbes, and total bilirubin in primary sclerosing cholangitis
- PMID: 39624235
- PMCID: PMC11609371
- DOI: 10.1016/j.jhepr.2024.101188
Fecal deoxycholic acid associates with diet, intestinal microbes, and total bilirubin in primary sclerosing cholangitis
Abstract
Background & aims: Primary sclerosing cholangitis (PSC) is a chronic cholestatic liver disease with a strong association with inflammatory bowel disease and variable disease progression. We aimed to gain insights into the role of fecal bile acids (BA) on disease progression by determining the relationships between fecal BA, diet, and gut microbes, with markers of disease progression, BA synthesis, and farnesoid X receptor (FXR) activity.
Methods: BA levels in serum and stool, dietary intake, and markers of BA synthesis, and FXR activity were measured in 26 patients with early stage, large duct PSC. Fecal microbiota were quantified by 16S rRNA gene sequencing.
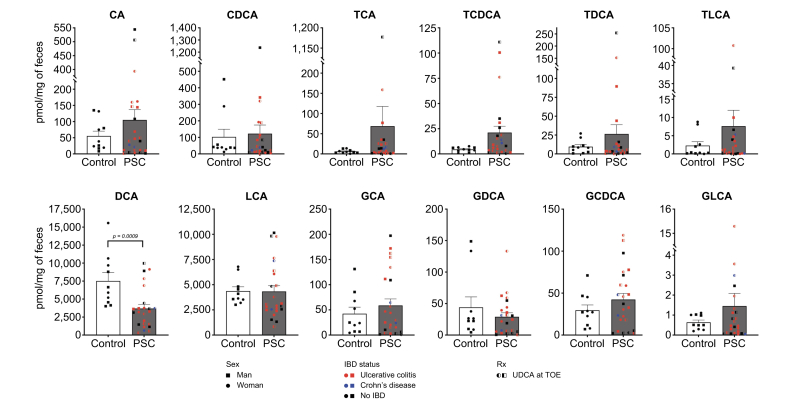
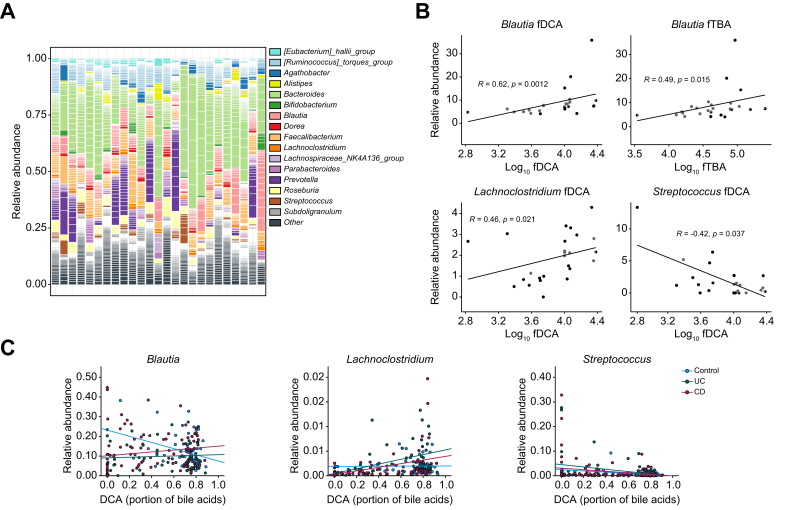
Results: Compared with controls, fecal unconjugated deoxycholic acid (DCA) levels were lower in patients with PSC (p adj = 0.04). Alcohol intake and the abundance of Blautia and Lachnoclostridium were associated with greater fecal DCA levels in patients with PSC after adjusting for inflammatory bowel disease and treatment with ursodeoxycholic acid. Fecal DCA levels were negatively associated with total bilirubin levels in patients with PSC (p = 0.006) suggesting a protective role. However, fecal DCA was associated with greater serum levels of 7α-hydroxy-4-cholesten-3-one, a marker of BA synthesis, and was not associated with fibroblast growth factor 19, a marker of intestinal FXR activity.
Conclusions: Alcohol intake, Blautia and Lachnoclostridium abundance was associated with increased fecal DCA levels, which in turn seemed to have had a protective effect in patients with early-stage PSC. However, this effect was not mediated by BA synthesis or FXR activation.
Impact and implications: Primary sclerosing cholangitis (PSC) is a cholestatic liver disease with a direct interaction between the gut and the liver. In this study of patients with early-stage PSC, levels of fecal deoxycholic acid correlated with serum total bilirubin, a marker of clinical outcomes. In addition, Blautia and Lachnoclostridium were associated with fecal deoxycholic acid suggesting an interaction between these gut bacteria, fecal bile acids, and disease progression. Future research to determine the underlying mechanisms of these associations may lead to novel targets to prevent PSC disease progression.
Keywords: Bile acids; Cholestatic liver disease; Diet; Disease progression; Microbes.
© 2024 The Author(s).
Conflict of interest statement
CC, ML, PF, WG, RD, MY, JZ, M-CV, OB, MT declare no conflicts of interest related to this manuscript. MT received grant support from Albireo, Alnylam, Cymabay, Falk, Gilead, Intercept, MSD, Takeda and UltraGenyx; honoraria for consulting from Abbvie, Albireo, Boehringer Ingelheim, BiomX, Falk, Genfit, Gilead, Hightide, Intercept, Jannsen, MSD, Novartis, Phenex, Pliant, Regulus, Siemens and Shire; speaker fees from Albireo, Bristol-Myers Squibb, Falk, Gilead, Intercept, MSD and Madrigal, as well as travel support from AbbVie, Falk, Gilead and Intercept. He is also co-inventor on patents on the medical use of norUDCA/norucholic acid filed by the Medical University of Vienna. JRK is on the advisory board of Corevitas, Promakhos, Thetis, ClostraBio and Founder of Colonary Concepts, and Bilayer Therapeutics. MLM is on the scientific advisory board for Nura, USA. CLB has received grant/research support from Calliditas, Gilead, Intercept, Bristol Myers Squibb, GSK, Cour, Novo Nordisk, CymaBay, Genfit, Pliant, Boston Scientific, Viking, and Cara and has consulted for Ipsen, Pliant, Cymabay, and GSK. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures



References
-
- Bowlus C.L., Arrivé L., Bergquist A., et al. AASLD practice guidance on primary sclerosing cholangitis and cholangiocarcinoma. Hepatology. 2023;77:659–702. - PubMed
-
- Trivedi P.J., Bowlus C.L., Yimam K.K., et al. Epidemiology, natural history, and outcomes of primary sclerosing cholangitis: a systematic review of population-based studies. Clin Gastroenterol Hepatol. 2022;20:1687–1700.e4. - PubMed
