

Phase II Trial of Regorafenib and Oral Methotrexate in Previously Treated Advanced KRAS-Mutant NSCLC
- PMID: 39624248
- PMCID: PMC11609302
- DOI: 10.1016/j.jtocrr.2024.100741
Phase II Trial of Regorafenib and Oral Methotrexate in Previously Treated Advanced KRAS-Mutant NSCLC
Abstract
Introduction: There are no standard targeted treatment options for advanced KRAS-mutant NSCLC beyond KRAS G12C inhibitors. A computational model identified regorafenib and low-dose methotrexate as synergistic in preclinical models of KRAS-mutant NSCLC. This study evaluated the efficacy and safety of the combination in previously treated advanced KRAS-mutant NSCLC.
Methods: This single-arm phase II study included regorafenib 80 to 120 mg oral daily and oral methotrexate dose escalated to tolerability from 10 to 20 mg twice weekly during the first cycle. Both agents were administered on weeks 1 to 3 of each 4-week cycle. The primary end point was progression-free survival.
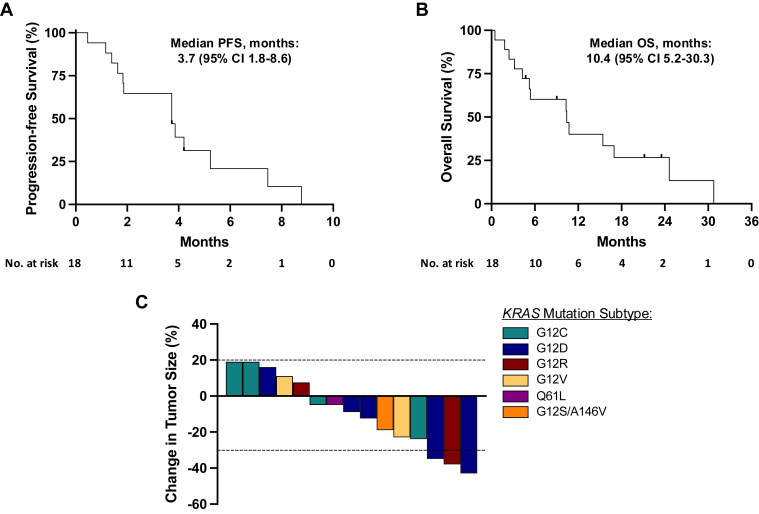
Results: In total, 18 patients with KRAS-mutant NSCLC were enrolled. Five patients received regorafenib at a 120 mg starting dose with four discontinuing due to toxicity; subsequently, 13 patients were treated at an 80 mg starting dose, with eight dose-escalating to 120 mg after the first cycle. Median progression-free survival was 3.7 months (95% confidence interval 1.8-8.6) and median overall survival was 10.4 months (95% confidence interval 5.2-30.3). The objective response rate was 16.7% and the 8-week disease control rate was 66.7%. Grade 3 treatment-related adverse events occurred in 11 patients, most often oral mucositis (n = 2) and asymptomatic lipase increase (n = 2). One patient developed asymptomatic grade 4 lipase increase.
Conclusions: Combination treatment of regorafenib and oral methotrexate in patients with KRAS-mutant NSCLC was limited due to toxicity, and the study did not meet its primary end point. Computational modeling may aid in repurposing therapeutic options though caution must be exercised with tolerability.
Keywords: KRAS mutation; Methotrexate; Regorafenib; Targeted therapy; ctDNA.
© 2024 The Authors.
Conflict of interest statement
Dr. Aredo reports receiving consulting fees from AstraZeneca. Dr. Wakelee reports receiving study support from Bayer Pharmaceuticals; receiving grants to institution from AstraZeneca/Medimmune, Bayer, Bristol Myers Squibb, Genentech/Roche, Helsinn, Merck, SeaGen, and Xcovery; receiving consulting fees from IOBiotech, OncoC4, and Beigene; and having participation on a data safety monitoring board for Mirati. Dr. Neal reports receiving grants to institution from Genentech/Roche, Merck, Novartis, Boehringer Ingelheim, Exelixis, Nektar Therapeutics, Takeda Pharmaceuticals, Adaptimmune, GlaxoSmithKline, Janssen, and AbbVie; consulting fees from AstraZeneca, Genentech/Roche, Exelixis, Takeda Pharmaceuticals, Eli Lilly and Company, Amgen, Iovance Biotherapeutics, Blueprint Pharmaceuticals, Regeneron Pharmaceuticals, Natera, Sanofi/Regeneron, D2G Oncology, Surface Oncology, Turning Point Therapeutics, Mirta Therapeutics, Gilead Sciences, AbbVie, Summit Therapeutics, Novartis, Novocure, Janssen Oncology, Anheart Therapeutics, and Bristol Myers Squibb; and honoraria from CME Matters, Clinical Care Options CME, Research to Practice CME, Medscape CME, Biomedical Learning Institute CME, MLI PeerView CME, Prime Oncology CME, Projects in Knowledge CME, Rockpointe CME, MJH Life Sciences CME, Medical Educator Consortium, and HMP Education. Dr. Diehn reports receiving grants from 10.13039/100004325AstraZeneca and 10.13039/100007210Varian Medical Systems; receiving royalties from Roche, Foresight Diagnostics, and Celgene; receiving consulting fees from AstraZeneca, Genentech, Gritstone Bio, Illumina, and Regeneron; receiving honoraria from Bristol Myers Squibb and Novartis; receiving support for meetings/travel from Foresight Diagnostics and Regeneron; having patent filings on ctDNA detection assigned to Stanford University and licensed to Roche or Foresight Diagnostics; having patent filings on single-cell analysis methods assigned to Stanford University and licensed to Celgene; having board member role in Foresight Diagnostics; having stocks in CiberMed, Foresight Diagnostics, Gritstone Bio, and Perception Medicine; and serving as invited faculty at Hokkaido University. Dr. Salahudeen reports receiving consulting fees from 10X Genomics, Droplet, and Pharmacosmos and was a former Tempus Labs employee. Dr. Kwong reports receiving consulting fees from Novocure. Dr. Vali reports having stocks in Cellworks Group Inc. and was a former employee of Cellworks Group Inc. Dr. Padda reports receiving grants to institution from Bayer, EpicentRx, Boehringer-Ingelheim, Bioalta, Takeda, and Amgen; serving on the advisory board of Takeda, AstraZeneca, Bayer, Amgen, Sanofi Genzyme, Rayze Biotech, Mirati, Janssen, Regeneron, Jazz Pharmaceuticals, Genentech, Nanobiotix, G1 therapeutic, Blueprint, Pfizer, and AbbVie; and receiving honoraria from PER, Curio Science LLC, MECC Global Meetings, and CME Solutions. All remaining authors have declared no conflicts of interest.
Figures
References
-
- Jänne P.A., Riely G.J., Gadgeel S.M., et al. Adagrasib in non-small-cell lung cancer harboring a KRASG12C mutation. N Engl J Med. 2022;387:120–131. - PubMed
-
- de Langen A.J., Johnson M.L., Mazieres J., et al. Sotorasib versus docetaxel for previously treated non-small-cell lung cancer with KRASG12C mutation: a randomised, open-label, phase 3 trial. Lancet. 2023;401:733–746. - PubMed
-
- Kies M.S., Christensen O., Lin T., et al. Phase I study of regorafenib (BAY 73–4506), an inhibitor of oncogenic and angiogenic kinases, administered continuously in patients (pts) with advanced refractory non-small cell lung cancer (NSCLC) J Clin Oncol. 2010;28
-
- Selawry O., Krant M., Scotto J., et al. Methotrexate compared with placebo in lung cancer. Cancer. 1977;40:4–8. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
