

Phenotypes of South Asian patients with atrial fibrillation and holistic integrated care management: cluster analysis of data from KERALA-AF Registry
- PMID: 39624353
- PMCID: PMC11609390
- DOI: 10.1016/j.lansea.2024.100507
Phenotypes of South Asian patients with atrial fibrillation and holistic integrated care management: cluster analysis of data from KERALA-AF Registry
Abstract
Background: Patients with atrial fibrillation (AF) frequently experience multimorbidity. Cluster analysis, a machine learning method for classifying patients with similar phenotypes, has not yet been used in South Asian AF patients.
Methods: The Kerala Atrial Fibrillation Registry is a prospective multicentre cohort study in Kerala, India, and the largest prospective AF registry in South Asia. Hierarchical clustering was used to identify different phenotypic clusters. Outcomes were all-cause mortality, major adverse cardiovascular events (MACE), and composite bleeding events within one-year follow-up.
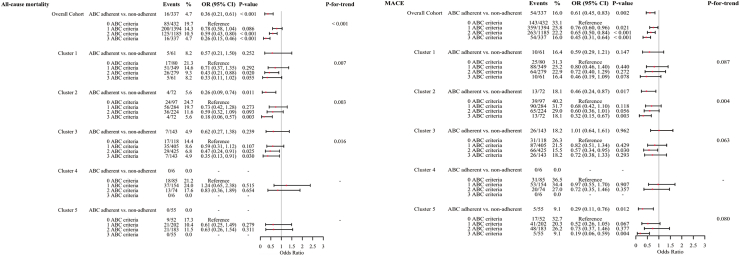
Findings: 3348 patients were included (median age 65.0 [56.0-74.0] years; 48.8% male; median CHA2DS2-VASc 3.0 [2.0-4.0]). Five clusters were identified. Cluster 1: patients aged ≤65 years with rheumatic conditions; Cluster 2: patients aged >65 years with multi-comorbidities, suggestive of cardiovascular-kidney-metabolic syndrome; Cluster 3: patients aged ≤65 years with fewer comorbidities; Cluster 4: heart failure patients with multiple comorbidities; Cluster 5: male patients with lifestyle-related risk factors. Cluster 1, 2 and 4 had significantly higher MACE risk compared to Cluster 3 (Cluster 1: OR 1.36, 95% CI 1.08-1.71; Cluster 2: OR 1.79, 95% CI 1.42-2.25; Cluster 4: OR 1.76, 95% CI 1.31-2.36). The results for other outcomes were similar. Atrial fibrillation Better Care (ABC) pathway in the whole cohort was low (10.1%), especially in Cluster 4 (1.9%). Overall adherence to the ABC pathway was associated with reduced all-cause mortality (OR 0.26, 95% CI 0.15-0.46) and MACE (OR 0.45, 95% CI 0.31-0.46), similar trends were evident in different clusters.
Interpretation: Cluster analysis identified distinct phenotypes with implications for outcomes. There was poor ABC pathway adherence overall, but adherence to such integrated care was associated with improved outcomes.
Funding: Kerala Chapter of Cardiological Society of India.
Keywords: ABC pathway; Atrial fibrillation; Clustering analysis; Kerala; Phenotype classification; South Asia.
© 2024 The Author(s).
Conflict of interest statement
All authors report no conflicts of interest.
Figures





References
-
- Kang D.-S., Yang P.-S., Kim D., et al. Racial differences in ischemic and hemorrhagic stroke: an ecological epidemiological study. Thromb Haemost. 2024;124(9):883–892. - PubMed
-
- Joglar J.A., Chung M.K., Armbruster A.L., et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. J Am Coll Cardiol. 2024;83(1):109–279. - PMC - PubMed
-
- Romiti G.F., Proietti M., Bonini N., et al. Clinical complexity domains, anticoagulation, and outcomes in patients with atrial fibrillation: a report from the GLORIA-AF registry phase II and III. Thromb Haemostasis. 2022;122(12):2030–2041. - PubMed
LinkOut - more resources
Full Text Sources
