

Cough in non-cystic fibrosis bronchiectasis
- PMID: 39624376
- PMCID: PMC11610066
- DOI: 10.1183/23120541.00330-2024
Cough in non-cystic fibrosis bronchiectasis
Abstract
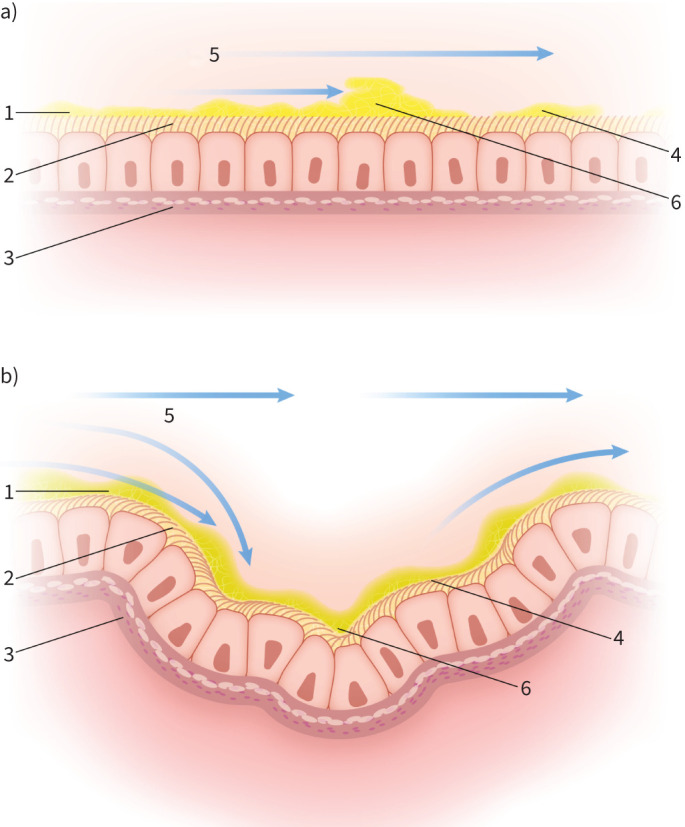
Non-cystic fibrosis bronchiectasis (NCFBE) belongs to the spectrum of chronic suppurative lung diseases and is characterised by persistent wet/sputum-productive cough and airway dilatation. Morphological and structural changes in the airways lead to changes in airflow, impair breathing-induced mucus transport and sliding, and reduce the shear forces of cough. Moreover, mucus hyperviscosity contributes to compromised ciliary activity and the pathogenesis of the disease. This mini-review highlights the role of cough in NCFBE, especially with respect to mucus clearance. Cough is the principal backup mechanism when mucus clearance is impaired due to either reduced function of cilia- and breathing-induced mucus transport, or abnormal mucus, or both. The efficiency of cough in overcoming the cohesive and adhesive properties of mucus is determined by both the forces applied to mucus by airflow and the mucus-airway surface properties. In NCFBE, mucus hyperviscosity contributes to impaired mucus clearance and determines disease pathogenesis; therefore, it may be a therapeutic target. The primary objectives of physiotherapy regimens in NCFBE are mucus hydration and the establishment of an optimal expiratory airflow velocity, which exerts shearing forces on the mucus located on the airway surface. Modifying the rheological properties of mucus and enhancing its transport whenever possible (by breathing manoeuvres, ciliary activity and cough) represent prime goals in preventing disease progression and, indeed reversing, bronchiectasis in the early stages of the disease, as well as preventing pulmonary exacerbations.
Copyright ©The authors 2024.
Conflict of interest statement
Conflict of interest: A. Kantar is currently serving as an Associate Editor for ERJ Open Research. W-J. Song is currently serving as Chief Editor for ERJ Open Research. The remaining authors have nothing to disclose.
Figures
References
LinkOut - more resources
Full Text Sources