

The progress of mother-to-child transmission of Human Immunodeficiency Virus (HIV) after Dolutegravir (DTG) optimization program: evidence from a multicenter cohort study in Ethiopia
- PMID: 39627710
- PMCID: PMC11613881
- DOI: 10.1186/s12889-024-20761-w
The progress of mother-to-child transmission of Human Immunodeficiency Virus (HIV) after Dolutegravir (DTG) optimization program: evidence from a multicenter cohort study in Ethiopia
Abstract
Background: Ethiopia aims to eliminate mother-to-child transmission (MTCT) of HIV by 2030. In 2020, Dolutegravir-based antiretroviral treatment (ART) regimen optimization was done for the Prevention of Mother-to-Child Transmission (PMTCT). However, data tracking progress, particularly post-rollout of the Dolutegravir (DTG)-based regimen, and the real-world effectiveness of the new regimen are unavailable.
Methods: A multicenter retrospective cohort study was conducted among HIV-infected mothers and their HIV-exposed infants visiting the selected hospitals for routine care. Eligible participants were HIV-exposed infants enrolled in the PMTCT care from 2017 to 2022. However, only the 2021 and 2022 birth cohorts were considered post-DTG optimization considering 2020 a year of optimization. The cumulative incidence of perinatal MTCT tested at 6-8 weeks of infant age, and end of care MTCT tested at 18 months of age was assessed. The exposures of the study were the infant birth cohort years and the different ART regimens used for PMTCT of HIV.
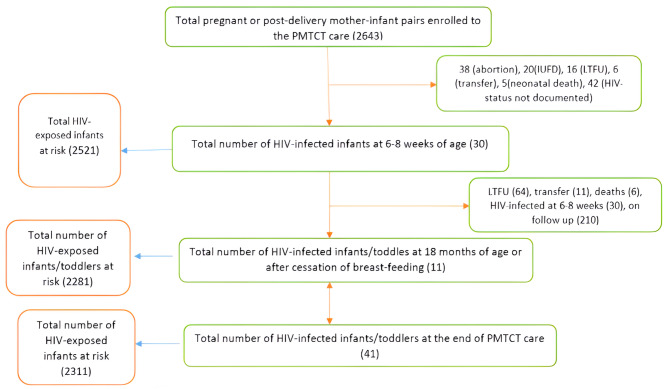
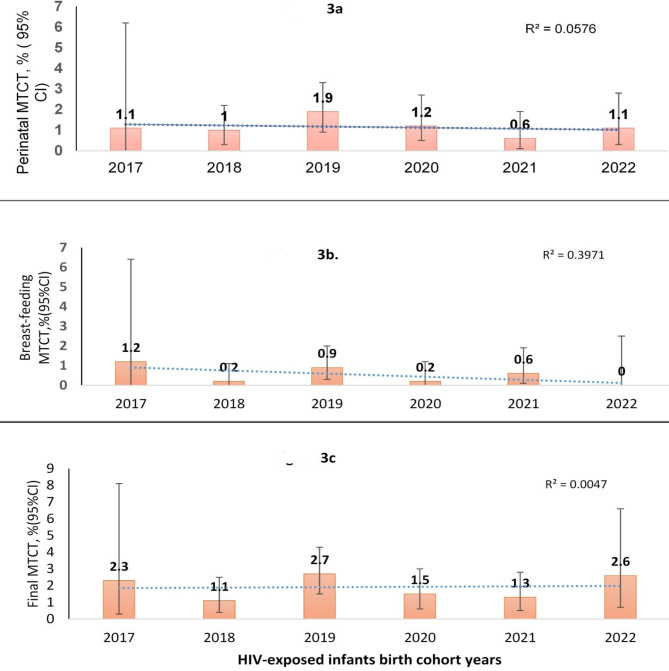
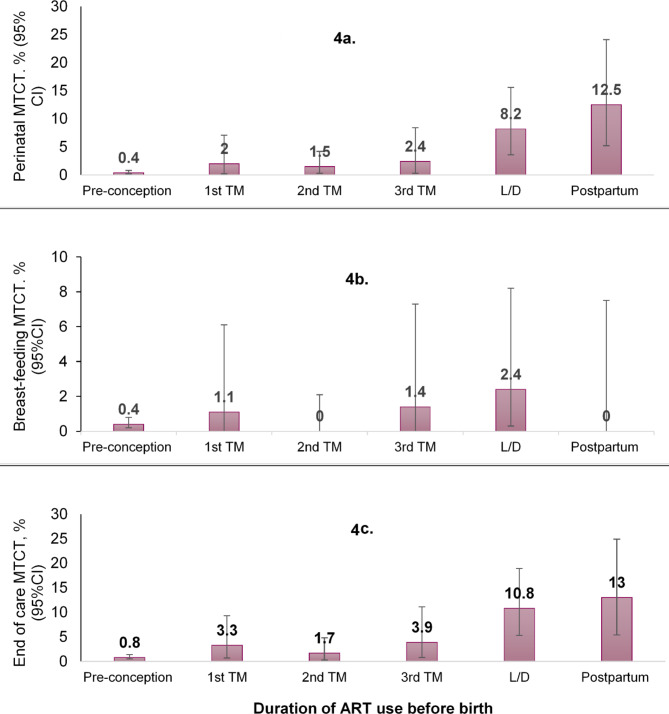
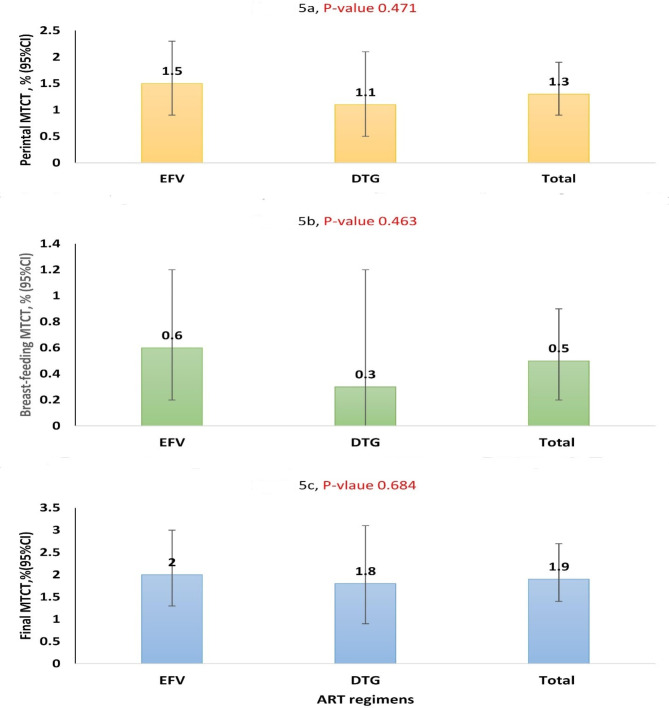
Results: Among a total of 2,643 routine care enrolled participants, 2521 (95.4%) HIV-exposed infants were included in the analysis. Of these, 210 were on follow-up and excluded from the breastfeeding MTCT analysis. A total of 30/2521(1.2%) [95% confidence interval (CI): 0.8-1.7%] were positive for HIV at 6-8 weeks. Additionally, 11 /2281 (0.50%) (95% CI: 0.3-0.9%) were positive during breastfeeding. At the end of the care, 41/2311 (1.8%) (95% CI: 1.3-2.4%) infants were HIV-positive. The highest end-of-care MTCT was reported in 2019 and 2022 birth cohorts while the lowest was in 2018 (P-value > 0.3). However, after adjusting for baseline characteristics, the trend showed a decrease in transmission rates following the rollout of DTG-based regimen, although statistical significance was not reached. The adjusted odds ratios (AORs) for perinatal, breastfeeding, and end-of-care transmission rates were 0.34 (95%CI: 0.08-1.39), 0.29(95%CI: 0.03-3.05), and 0.38(95%CI: 0.11-1.26) respectively. Compared with the Efavirenz (EFV)-based regimen, the DTG-based regimen was associated with a lower risk of MTCT in both the perinatal (AOR 0.23, 95% CI: 0.06-0.85) and at the end of care (AOR 0.27, 95% CI: 0.09-0.82). Pregnant women who started ART at late gestation had the highest transmission rate regardless of ART regimens (P-value < 0.001).
Conclusions: In the studied cohort population, we observed less than 3% MTCT rate at the end of PMTCT care. The findings might suggest the achievement of MTCT elimination at the hospital level. Although the DTG-based regimen demonstrated a lower risk of transmission, other contributing factors, such as late ART initiation, should be urgently addressed. Future research should focus on prospective designs, interventions targeting late ART initiation, and understanding regional disparities to further advance efforts to eliminate MTCT by 2030.
Keywords: Dolutegravir; Ethiopia; PMTCT; Pregnancy.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethics approval and consent to participate: Ethical approval was obtained from the ethical review boards of the Hawassa University College of Medicine and Health Sciences institutional review board (IRB), with reference number (IRB/076/2022, dated December 10/2022). The members of the ethics committee include Dr. Embiale Mengiste, Dr. Muhammed Ayalew and Dr. Freshet Assefa. Informed consent was waived based on the use of anonymized data from routine healthcare records. Data sharing: All data relevant to the study are included in this manuscript. Ethics approval and consent to participate: Ethical approval was obtained from the ethical review boards of the Hawassa University College of Medicine and Health Sciences institutional review board (IRB). The members of the ethics committee include Dr. Embiale Mengiste, Dr. Freshet Asefa, Dr. Muhammed Ayalew. Informed consent was waived based on the use of anonymized data from routine healthcare records. Consent for publication: not applicable Patient and public involvement: Patients or the public were not involved in the design, or conduct, or reporting. However, we will involve the public or stakeholders during dissemination of the result.
Figures
References
-
- Kourtis AP, Bulterys M. Mother-to-child transmission of HIV: pathogenesis, mechanisms and pathways. Clin Perinatol. 2010;37(4):721–37. - PubMed
-
- Kourtis AP, Lee FK, Abrams EJ, Jamieson DJ, Bulterys M. Mother-to-child transmission of HIV-1: timing and implications for prevention. Lancet Infect Dis. 2006;6(11):726–32. - PubMed
-
- De Cock KM, Fowler MG, Mercier E, De Vincenzi I, Saba J, Hoff E, et al. Prevention of mother-to-child HIV transmission in resource-poor countries: translating research into policy and practice. JAMA. 2000;283(9):1175–82. - PubMed
-
- WHO. PMTCT strategic vision 2010–2015: preventing mother-to-child transmission of HIV to reach the UNGASS and Millennium Development Goals: moving towards the elimination of paediatric HIV, 2009. 2010.
-
- UNAIDS. Miles to go: closing gaps, breaking barriers, righting injustices. 2018.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
