

Evaluation of response to a cholera outbreak in January 2024 using the 7-1-7 timeliness metrics: a case study of Elegu Point of Entry, Uganda
- PMID: 39627766
- PMCID: PMC11616103
- DOI: 10.1186/s12889-024-20886-y
Evaluation of response to a cholera outbreak in January 2024 using the 7-1-7 timeliness metrics: a case study of Elegu Point of Entry, Uganda
Abstract
Background: Cholera is a major public health threat in Uganda, especially in border districts prone to outbreaks from cross-border movement. We investigated and evaluated the initial response to a January 2024 cholera outbreak in Elegu Town, on the Uganda-South Sudan border, using the 7-1-7 timeliness metrics to assess detection, notification, and response capacities, highlighting Uganda's preparedness and challenges in managing cross-border outbreaks.
Methods: We defined a suspected case as the onset of acute watery diarrhea in an asylum seeker at the Elegu border point from January to February 2024. A confirmed case was a suspected case in which Vibrio cholerae was isolated in the stool by culture or PCR. We actively searched for cases and collected data on person characteristics, symptoms, and outbreak timeliness. We used semi-structured interviews to elicit insights from district health officials on the enabling factors and bottlenecks during the response. We used the 7-1-7 metric to assess detection, notification, and response capacities of the point of entry.
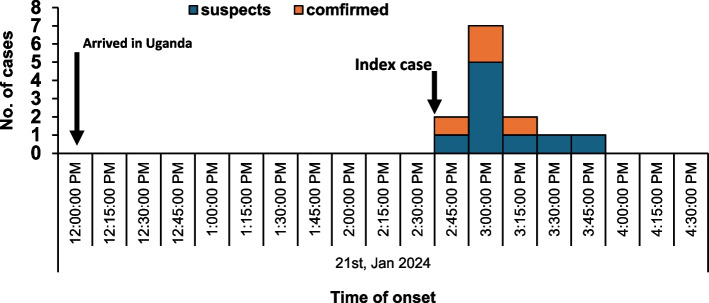
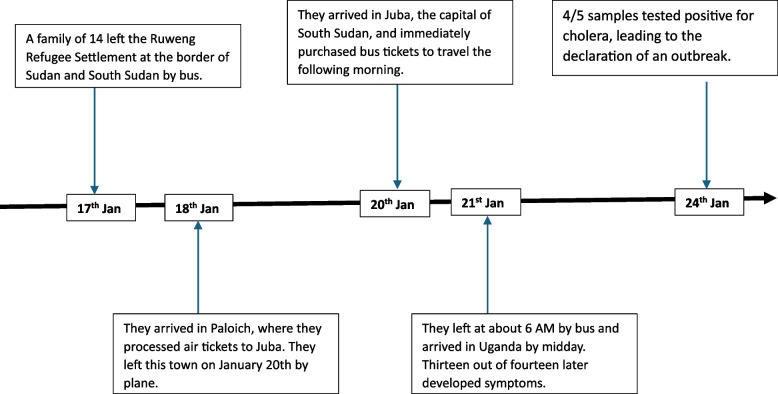
Results: Thirteen members of a refugee family from South Sudan were diagnosed with cholera within 6 h of arrival at the Elegu border, with 4 (31%) confirmed cases. No death occurred. The authorities detected, notified, and responded to the outbreak within the 7-1-7 timelines, with no major bottlenecks identified. The outbreak was detected and notified within one day and by the fifth day, a full response was mounted. The prompt response was attributed to the availability of a functional emergency operations center and the presence of trained surveillance frontline health workers.
Conclusion: Response to an imported cholera outbreak at Elegu border point demonstrated Uganda's preparedness in managing cross-border disease outbreaks. Achieving the 7-1-7 targets highlighted the country's-built capacity to detect, notify, and respond to such events. Continued investment in local-level disease detection, communication, and national-level resource mobilization will be crucial to sustaining future effective cross-border outbreak prevention and control strategies.
Keywords: 7–1–7 metrics; Cholera; Cross-border outbreak prevention and control; Detection; Imported outbreak; Notification; Response; Uganda.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: We conducted this study in response to a public health emergency and as such it was determined to be non-research. The MoH authorized this study and the office of the Center for Global Health, US Center for Disease Control and Prevention determined that this activity was not human subject research and with its primary intent being for public health practice or disease control. This activity was reviewed by CDC and was conducted consistent with applicable federal law and CDC policy. §§See e.g., 45 C.F.R. part 46, 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq. We obtained permission to investigate from the Adjumani District health authorities and the Nyumanzi Refugee Settlement authorities. We obtained verbal consent from all the respondents aged ≥ 18 years since all the patients were under isolation at time of this investigation. For those aged < 18 years, we obtained consent from the parents and assent from the respondents. Participants were assured that their participation was voluntary and that there would be no negative consequences for declining participation in the investigation. Data collected did not contain any individual personal identifiers and information was stored in password-protected computers, which were inaccessible to anyone outside the investigation team. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Bhattacharya SK, Nair GB, Takeda Y. Renewed Interest in Cholera Control. J Gastroenterol Hepatol Rep. 2022;3(1):1–5.
-
- Erkyihun GA, Asamene N, Woldegiorgis AZ. The Threat of Cholera in Africa. Zoonoses. 2023;3(1):20230027.
-
- Mengel, M.A., et al., Cholera outbreaks in Africa. Cholera outbreaks; 2014: p. 117–144. - PubMed
-
- Echenberg, M., Africa in the Time of Cholera: A History of Pandemics from 1817 to the Present. Cambridge University Press; 2011. Vol. 114 .
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
